Hospital-at-home programs have expanded rapidly across the U.S., but most patients have no idea this option exists when facing admission.
When my husband George was cycling through hospital stays every month for his end-stage renal disease and cancer in 2018, nobody told us there might be another way. We assumed the hospital was our only option. Month after month, we dealt with the ER waits, the uncomfortable chairs, the sleepless nights, and the parade of specialists who never seemed to talk to each other.
Things have changed since then. Hospital-at-home care has gone from experimental to mainstream. Medicare now covers it permanently. Your insurance probably covers it too.
But you have to know to ask for it.
Let’s break down everything you need to know about hospital-at-home versus traditional hospitalization, including:
a comparison of clinical outcomes
the hidden costs nobody talks about
how to decide which option makes sense for your situation
Hospital-at-home means exactly what it sounds like: you receive acute-level medical care in your own home instead of in a hospital facility. This isn’t the same as regular home healthcare or skilled nursing. We’re talking about the same intensity of care you’d get if you were admitted to a hospital bed.
What conditions qualify for hospital-at-home care?
The key word here is “acute.” You need to be sick enough to require hospitalization, but stable enough to be safely monitored at home.
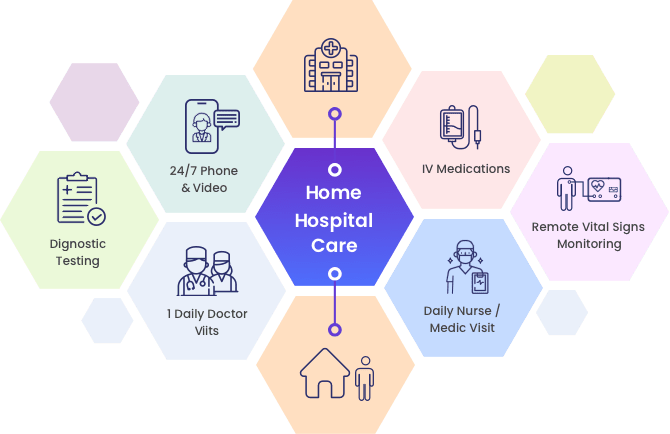
What does hospital-level care actually include?
Your care team visits you at home daily, and sometimes twice a day. This includes physicians, nurses, physical therapists, and care coordinators. You’ll get IV medications if you need them. You’ll wear devices that monitor your vital signs and send data to your medical team in real-time. It’s like having a hospital room set up in your living room, but without the hospital smell and terrible food.
When George was using his Dexcom continuous glucose monitor, I got alerts on my phone whenever his blood sugar spiked or dropped dangerously low. That technology exists for heart rate, oxygen levels, blood pressure, and more. Your care team watches these numbers from their computers and can intervene before small problems become emergencies.
Who provides the care?
A dedicated hospital-at-home team manages your case. You’ll have a primary physician who oversees your treatment plan. Nurses visit to check on you, administer medications, and assess your condition. The big difference from traditional home health? These visits happen daily, and you have 24/7 access to your care team by phone or video.
When you’re admitted to a traditional hospital, you check in through the emergency department or for a scheduled admission. A nurse takes your vitals, you change into a hospital gown, and you’re assigned to a room (if one’s available—sometimes you wait for hours).
The hospital routine
Nurses check your vitals every few hours, day and night. Yes, even at 3 a.m. Doctors round in the morning, usually between 7 and 10 AM. If you’re asleep when they come by, too bad. Meals arrive on a fixed schedule whether you’re hungry or not.
With George’s 10 different specialists, we never knew who would walk through the door or when. His nephrologist didn’t talk to his oncologist. His endocrinologist had no idea what his cardiologist prescribed. I became the central hub of information, keeping my own spreadsheet because the hospital’s electronic records didn’t seem to connect the dots.
Family involvement and visiting limitations
Even before COVID-19 restrictions, hospitals limited visiting hours. During the pandemic, many hospitals banned visitors entirely. In 2025, most facilities still have restrictions like limited hours, limited number of visitors, no children under 12.
If you want to be there when doctors round to ask questions, you’d better arrive early and stay all day.
Need to go home to shower or check on your kids? You might miss critical conversations about your loved one’s treatment plan.
That’s not surprising. People sleep better when they’re in their own beds. They get to eat their own food, and see their family members whenever they want.
The medical care is just as good, but the experience is dramatically better.
Hospital readmission rates
Getting sent back to the hospital within 30 days of discharge is a sign something went wrong.
That’s because closer monitoring catches problems earlier. Patients understand their care plan better because they’re not overwhelmed and sleep-deprived. The transition from acute care to regular life is smoother when you’re already home.
The mortality rates? Comparable. For appropriate patients, hospital-at-home is just as safe as traditional hospital care.
The Hidden Costs Nobody Tells You About
The hospital bill is just the beginning. Let’s talk about what you’ll actually pay and what costs don’t show up on an invoice.
Out-of-pocket expenses for traditional hospitalization
Even with good insurance, a three-day hospital stay can cost you $1,500 to $3,000 in co-pays and deductibles. That’s the baseline. Then come the surprise charges.
Facility fees can add hundreds of dollars:
Labs processed by an out-of-network pathologist costs extra.
And let’s not forget parking. $15 per day adds up when you’re visiting daily for weeks. Hospital cafeteria meals for family members is $10 to $15 each.
These “small” costs can easily hit $500 to $1,000 for a typical hospital stay.
Out-of-pocket expenses for hospital at home
Medicare covers hospital-at-home the same way it covers traditional hospitalization. You pay the standard hospital deductible and any applicable co-pays. Most private insurers follow Medicare’s lead, but coverage varies.
The surprise? Hospital-at-home often costs you less out-of-pocket because there’s no:
You might need to buy a few things—maybe a shower chair or grab bars if you don’t have them. But the program provides equipment like IV poles and monitoring devices.
The invisible costs for caregivers
The economic impact on caregivers is often overlooked. I burned through my vacation days and sick leave taking George to appointments and managing his care, even while working remotely. Many caregivers do the same.
Both hospital settings require serious caregiver involvement, just in different ways.
Caregiving during traditional hospitalization
You become an advocate and information manager. When doctors round at 8 a.m. and you can’t be there because you have a job, you miss critical conversations. So you take time off. You show up early. You stay late.
I kept notes from every specialist visit, cross-referenced medications, and flagged contradictions. The nutritionist told George to eat high-protein foods for his kidney disease. The renal dietitian told him to eat low-protein foods for his kidney disease. Guess who had to figure that out?
You’re also managing communication with the rest of the family. Who’s visiting when? Who needs updates? Coordinating schedules becomes a part-time job.
Caregiving with hospital at home
At home, you’re more hands-on with daily care:
You help your loved one to the bathroom.
You make sure they eat.
You learn to manage medications (when to give them, and spot side effects)
The medical team trains you. They don’t just hand you a list of tasks and disappear. They show you how to help with care, what to watch for, and when to call for help.
When I was managing George’s peritoneal dialysis at home, his nephrologist’s team trained me thoroughly. I set up the machine every night, monitored the process, troubleshot issues.
It was a big responsibility, but I wasn’t alone. I had 24/7 access to the dialysis team by phone.
The benefits of hospital-at-home care:
You have more control over the environment
You can maintain some routine
You sleep in your own bed
The stress of feeling “on call” is real, but many caregivers prefer it to feeling helpless in a hospital where they can’t be present all the time.
How to Know if Hospital at Home is Right for Your Situation
Hospital-at-home isn’t for everyone. Here’s how to figure out if it makes sense for you.
Medical eligibility criteria
Your condition needs to be serious enough to require hospitalization but stable enough to monitor at home. This includes conditions like:
Pneumonia (non-ICU level)
Heart failure exacerbations
COPD flare-ups
Cellulitis and other serious infections
Certain post-surgical recoveries
You don’t qualify if you need ICU-level care, constant monitoring, or procedures that can only be done in a hospital. You also need to live within 30 minutes of the hospital in case you need emergency transfer.
Home environment assessment
You need a space for medical equipment, like a corner where an IV pole can stand and monitoring equipment can plug in.
If you’re taking advantage of telehealth, you’ll also need reliable internet for video visits and data transmission and a phone.
Safety matters too. Can you get to the bathroom safely? Are there trip hazards that could cause falls? A nurse will assess your home before admission to make sure it’s appropriate.
Insurance coverage check
Call your insurance company and ask these specific questions:
“What’s my co-pay compared to traditional hospitalization?”
“Do I need pre-authorization?”
“Which hospitals in my area participate in your hospital-at-home network?”
Get the answers in writing. Insurance representatives make mistakes, and you don’t want surprises later.
Family readiness factors
Someone needs to be home or nearby. Not necessarily 24/7, but available. The medical team handles the clinical care, but you need a person there to help with activities of daily living and to be present during visits.
Consider your other responsibilities:
Do you have young kids?
Other family members who need care?
A job with no flexibility?
Be honest about your capacity. There’s no shame in saying traditional hospitalization is the better fit for your situation.
How to Access Hospital-at-Home Programs
Most doctors won’t automatically offer this option. You have to ask for it.
When your doctor says you need to be admitted, ask: “Am I eligible for a hospital-at-home program?” If they say they don’t know or haven’t heard of it, ask them to check. Many physicians are still learning about these programs.
Call your insurance company before admission if possible. Verify coverage and get any necessary pre-authorizations. Some programs accept patients directly from the emergency department, which can save you hours in the ER waiting room.
To find hospitals offering hospital-at-home in your area, check the Medicare website’s Hospital Compare tool or call hospitals directly and ask if they participate in hospital-at-home programs.
Questions to Ask Before You Decide
Before you commit to hospital-at-home, get clear answers to these questions.
For your medical team:
“Am I medically stable enough for hospital-at-home?”
“What happens if my condition gets worse at night or on weekends?”
“How quickly can I be transferred to the hospital if needed?”
For the program coordinator:
“How many times per day will someone visit me?”
“Will I see the same nurses and doctors, or will it change?”
“What equipment will be in my home, and who maintains it?”
For your insurance:
“What will my total out-of-pocket cost be?”
“How many days of hospital-at-home care are covered?”
“Is there a limit to how many times I can use this benefit?”
For your family:
“What will I be responsible for as a caregiver?”
“What training will I receive?”
“Who can I call when I’m overwhelmed or unsure?”
Get these answers before you decide. Understanding what you’re signing up for prevents surprises and helps you plan.
Making the Right Choice for Your Family
Hospital-at-home delivers the same quality of clinical care as traditional hospitalization—sometimes better.
But the right choice depends on your medical situation, your home environment, your insurance coverage, and your family’s capacity to help with care.
If George had the option for hospital-at-home care during his treatment, would it have changed the outcome? Probably not. His conditions were too complex and unstable.
But it would have changed our experience. Fewer nights in uncomfortable hospital chairs. More time in our own home. Better sleep for both of us. For the right patient and the right family, those differences matter tremendously.
Know that you have options. Ask questions and advocate for yourself. Don’t assume the hospital is the only place to receive acute care, because it’s not.
If you’re facing hospitalization decisions for yourself or a loved one, share this information with your family. Ask your doctor about hospital-at-home before admission. You might be surprised by what’s possible.
Cryer, L., Shannon, S. B., Van Amsterdam, M., & Leff, B. (2023). Costs for Hospital at Home Patients Were 19 Percent Lower, With Equal or Better Outcomes Compared to Similar Inpatients. Health Affairs, 42(6), 861-868. Retrieved from https://pubmed.ncbi.nlm.nih.gov/22665835/
Edgar, K., Iliffe, S., Doll, H. A., Clarke, M.J., Gonçalves-Bradley, D.C., Wong E., & Shepperd, S. (2024). Admission avoidance hospital at home. Cochrane Database of Systematic Reviews. Mar 5;3(3):CD007491. doi: 10.1002/14651858.CD007491.pub3. Retrieved from https://pubmed.ncbi.nlm.nih.gov/38438116/
Federman, A. D., Soones, T., DeCherrie, L. V., Leff, B., & Siu, A. L. (2018). Association of a Bundled Hospital-at-Home and 30-Day Postacute Transitional Care Program With Clinical Outcomes and Patient Experiences. JAMA Internal Medicine. Aug 1;178(8):1033-1040. doi: 10.1001/jamainternmed.2018.2562. Retrieved from https://pubmed.ncbi.nlm.nih.gov/29946693/
HAI and Antimicrobial Use Prevalence Surveys. (2024). Centers for Disease Control. Retrieved from https://www.cdc.gov/healthcare-associated-infections/php/haic-eip/antibiotic-use.html
Horwitz, L. I., Moriarty, J. P., Chen, C., et al. (2020). Quality of discharge practices and patient understanding at an academic medical center. JAMA Internal Medicine, 180(8), 1125-1131. Retrieved from https://pubmed.ncbi.nlm.nih.gov/23958851/
Levine, D. M., Ouchi, K., Blanchfield, B., et al. (2023). Hospital-Level Care at Home for Acutely Ill Adults: A Randomized Controlled Trial. Annals of Internal Medicine, 176(11), 1455-1466. Retrieved from https://pubmed.ncbi.nlm.nih.gov/31842232/
The House spending bill dropped a bombshell for digital health companies: a proposed 5-year extension for hospital-at-home waivers and 2-year extension for Medicare telehealth flexibilities.
Five years sounds like forever in tech time. But it’s actually a strategic planning nightmare.
Do you build for temporary policy, or bet everything on permanence?
I spent 2 years managing care for my terminally ill husband across 10 different doctors. Every month, he landed back in the hospital with high A1C, low hemoglobin, unbearable pain. If hospital-at-home programs had existed in 2016 with the right technology backing them, he could have avoided dozens of ER visits.
Hospital at home is the future. The question is, what should Series A, B and C health tech founders build in the next 24 months that creates value regardless of what Congress does in 2030?
This isn’t about policy speculation. It’s about strategic planning with incomplete information—which is exactly what building a health tech company requires.
What the Proposed Funding Package Actually Changes
Source: Modern Healthcare
The proposed House spending bill extends two critical Medicare programs—but on very different timelines. Understanding these differences matters if you’re building technology in this space.
The 5-year hospital-at-home timeline explained
The proposed legislation would extend the hospital-at-home waiver through 2030. This isn’t just another short-term patch. Previous extensions gave health systems and tech companies 12-18 months of runway at best.
The current acute hospital care at home initiative lets Medicare pay for hospital-level services delivered in patients’ homes. Without the extension, this program expires in 2025. That’s not enough time to build, validate, and scale meaningful technology infrastructure.
Five years gives you real planning horizon. You can make legitimate platform investments. You can hire engineering teams. You can sign multi-year contracts with health systems.
But—and this is critical—5 years isn’t permanent. It’s a policy experiment with a longer fuse.
What’s still uncertain despite the extension
Even with a 5-year extension, huge questions remain unanswered. CMS hasn’t committed to specific reimbursement rates beyond the waiver period. Will hospital-at-home payments match facility-based acute care, or will they drop to home health rates?
State regulations vary wildly. Some states embrace home-based acute care. Others have licensing requirements that make it nearly impossible. Federal waivers don’t override state-level barriers.
Commercial payers watch Medicare but don’t automatically follow. Your hospital-at-home technology needs Medicare coverage to scale, but commercial adoption determines whether you build a sustainable business.
Technology requirements could shift too. CMS might mandate specific monitoring capabilities, interoperability standards, or quality reporting metrics that don’t exist yet.
Planning for 5 years means planning for uncertainty, not betting on stability.
Most Founders Are Asking the Wrong Question
When the House bill news broke, founder group chats exploded with one question: “Does this mean hospital-at-home is permanent?” That’s the wrong question. It reveals a misunderstanding of how health tech businesses actually succeed or fail.
“Is this permanent?” misses the strategic point
Policy permanence has never guaranteed health tech success. Remote patient monitoring has had Medicare coverage since 2019. Chronic care management codes have existed for years. Both have clear reimbursement pathways. Both have policy stability.
Yet most RPM companies struggle to achieve profitability. Many CCM platforms shut down despite favorable policy.
The real risk isn’t policy reversal. It’s building something nobody needs or can’t afford to operate. Investors price in regulatory risk and execution challenges unique to healthcare.
Your business model needs to create value across multiple scenarios. If hospital-at-home waivers expire in 2030, can your technology pivot to post-acute care? Skilled nursing facilities? Palliative care at home? If you’ve built exclusively for one reimbursement code, you’ve built a fragile company.
The trap of building exclusively for waivers
Remember the telehealth boom of 2020-2021? Some telehealth companies that scaled to thousands of employees during COVID laid off half their staff by 2023.
They weren’t bad companies. They built for a policy moment, not a durable market need.
VCs learned an expensive lesson: waiver-dependent revenue is risky revenue. When I talk to Series B investors now, they ask pointed questions. What percentage of your revenue requires temporary policy? If that policy changes, what’s your Plan B? Can you operate profitably under traditional Medicare rates?
If you can’t answer those questions convincingly, your valuation suffers—even if current policy looks favorable.
What “5 years” really means for your product roadmap
Five years is approximately two technology development cycles for complex healthcare platforms. You can ship an MVP, gather real-world evidence, iterate based on feedback, and launch a mature v2.0 product in that timeframe.
But 5 years isn’t enough time to build everything. You need to prioritize ruthlessly.
Your 24-month window is critical. This is when you validate product-market fit, prove unit economics, and establish your competitive moat. If you can’t demonstrate margin-positive cohorts by month 24, the next 3 years won’t save you.
Years 3 to 5 should assume policy uncertainty, not stability. Build optionality into your architecture. Make sure your platform can serve multiple care settings. Design your data infrastructure to support different payment models.
One scenario planning exercise: map out what your business looks like if hospital-at-home waivers expire in 2030 versus extend another 5 years vs. become permanent. If all three scenarios require fundamentally different strategies, you’re not building a durable company. You’re building a policy bet.
Your 24-Month Minimum Viable Stack
The next 2 years determine everything. You need to build technology that proves value quickly while laying foundation for longer-term expansion. Here’s where to focus your engineering resources and capital.
Core infrastructure that works across reimbursement models
Start with the basics that every home-based care model needs, regardless of how Medicare pays for it.
Remote patient monitoring devices need to integrate seamlessly with your platform. But don’t overbuild here. Start with FDA-cleared devices for vital signs (blood pressure, pulse ox, weight, glucose). Specialty monitoring for rare conditions can wait until you’ve proven your core model works.
Virtual triage and clinical communication platforms matter more than most founders realize. When a patient’s oxygen saturation drops at 3 a.m., someone needs to decide: send an ambulance, dispatch a nurse, or coach the patient through the moment remotely? That decision-making capability is what health systems pay for, not just the device data.
Care orchestration is the unsexy backbone nobody wants to build but everyone needs. Who schedules the nurse visit? Who orders medical supplies? Who coordinates with the patient’s primary care doctor? These back-office functions represent over half of the $1 trillion in annual U.S. healthcare waste. Automating them creates immediate ROI.
EHR integration isn’t optional. Payers demand it. Health systems require it. Your platform needs to pull patient data from Epic, Cerner, and other major EHRs, then push back visit notes, monitoring data, and care plans. Budget 20 to 30% of your engineering resources just for integration work.
Where to invest in AI right now
Source: Health Care Code
Ambient clinical intelligence (ACI) has reached near-universal adoption: 92% of health systems are piloting or deploying AI scribes. These tools improve documentation accuracy, leading to 10 to 15% revenue capture improvement through better coding and billing.
For hospital-at-home programs, this matters enormously. Nurses and paramedics doing home visits often struggle with documentation. They’re managing complex patients in unpredictable environments. AI that turns their verbal notes into structured clinical documentation saves 30 to 45 minutes per visit.
Predictive analytics should focus on preventing acute episodes that require hospitalization. Machine learning models can analyze vital sign trends, medication adherence patterns, and social determinants data to flag patients at risk of decompensation. One health system using predictive monitoring reduced readmissions by 23% in their hospital-at-home cohort—that’s the difference between a margin-positive program and one that loses money on every patient.
Don’t sleep on care coordination automation. If family caregivers spend 15-20 hours per week on caregiving tasks (as CareYaya Health Technologies data shows), your AI should reduce that burden. Automated medication reminders, appointment scheduling, and supply ordering aren’t flashy features, but they’re what caregivers desperately need.
The unsexy AI that saves money: Back-office automation in revenue cycle management, prior authorization, and claims integrity. These AI applications can reach 70-80% profit margins and generate $500K-$1M in annual recurring revenue per full-time employee. That cash flow funds your clinical AI development.
The Margin Math That Actually Matters
Most hospital-at-home programs lose money. Your technology needs to change that equation, or you don’t have a sustainable business.
Why most hospital-at-home programs lose money
Medicare pays $1,000 to $1,500 per day for hospital-at-home. Most programs spend $1,200 to $1,600 per patient daily on nurse visits, supplies, coordination, and tech. They’re underwater from Day 1.
The hidden costs kill you. Logistics and care orchestration require significant labor. Someone schedules visits, manages the supply chain, and coordinates with the patient’s other providers. Traditional staffing models don’t scale—you can’t apply facility-based nursing ratios to home care and expect it to work economically.
Technology that creates work instead of reducing it makes the problem worse. I’ve seen hospital-at-home platforms that require nurses to log into five different systems per visit. The documentation burden exceeds what they’d do in a hospital setting.
How AI makes care at home programs profitable
Revenue cycle optimization through better documentation can improve revenue capture by 10-15%. When a nurse describes a patient’s condition verbally and AI generates accurate, complete clinical notes with proper billing codes, you get paid more for the same work.
Source: MDhelpTEK
Reduced readmissions drive CMS quality bonuses. The hospital-at-home model already shows lower readmission rates than traditional acute care—adding predictive monitoring amplifies that advantage. Every readmission you prevent saves $10,000 to $15,000 in costs and protects against CMS penalties.
Labor cost reduction matters most. AI triage can cut nurse workload by 40%+ in pilot programs. Instead of nurses manually reviewing monitoring data for every patient, AI flags only the patients who need clinical attention. A nurse who previously managed 5-6 hospital-at-home patients can now manage 8 to 10.
The “unsexy” AI that CFOs love but VCs overlook: billing, coding, claims integrity. Administrative AI can reduce operational costs by 30-40%. That’s real margin improvement hitting your income statement immediately.
Proving ROI to your board in the next 6 months
Source: ScribeMD
Your board doesn’t care about utilization growth if you’re losing money on every patient. They care about these metrics:
Cost per episode: What does it actually cost you to manage one hospital-at-home patient from admission to discharge? Track this ruthlessly. Break it down by component: labor, supplies, technology, overhead.
Readmission rates: Hospital-at-home programs typically achieve 8 to 12% 30-day readmission rates versus 15 to 18% for traditional hospital care. If your program doesn’t beat facility-based benchmarks, you have a quality problem.
Patient satisfaction: CMS increasingly ties reimbursement to patient experience scores. Hospital-at-home programs score 15-20 points higher on patient satisfaction versus facility care. That’s your competitive advantage.
Structure pilot programs that generate defensible data. Work with 2 to 3 health systems willing to share financial and outcomes data transparently. You need to prove your technology improves margins, not just clinical outcomes.
The difference between utilization metrics and profitability metrics: lots of patients using your platform means nothing if each one loses money. Focus on contribution margin per patient. When does that number go positive? What’s the path to 40 to 50% gross margins?
The 3 to 5 Year Platform Expansion Strategy
Once you’ve proven your core model works and generates positive margins, you can think bigger. The next phase is about expanding beyond your initial use case.
From point solution to platform
Bessemer’s State of Health AI report describes “supernova” companies that achieve 6-10x growth trajectories by expanding from single point solutions into comprehensive platforms. Ambient scribes became full clinical documentation suites. Prior authorization tools became complete utilization management platforms.
The pattern:
Start with a painful, well-defined problem.
Solve it better than anyone else.
Expand into adjacent workflows that touch the same users.
For hospital-at-home technology, that might mean starting with post-surgical patients recovering at home. Prove you can manage that population safely and profitably. Then expand to heart failure management, COPD exacerbations, cellulitis treatment, chemotherapy administration.
Each expansion requires clinical validation and new reimbursement navigation. But your core technology infrastructure of monitoring, triage, care coordination, documentation stays largely the same.
Value-based care integration timeline
Source: Activated Insights
Hospital-at-home is a wedge into value-based care contracts, not just fee-for-service reimbursement. Accountable Care Organizations (ACOs) and Medicare Advantage plans care deeply about reducing avoidable hospitalizations. If your platform keeps patients out of expensive facility-based care, ACOs will pay for it.
But commercial adoption lags Medicare by 18 to 24 months historically. Don’t expect widespread MA plan adoption until 2027 to 2028, even with favorable hospital-at-home policy.
Self-insured employers represent a faster path to commercial revenue. Large employers pay directly for employee healthcare. When they see data showing hospital-at-home reduces costs by 30-40% versus facility admissions, they’ll write checks. Companies like Cubby, who secured $63 million in Series A funding led by Guggenheim Partners, are targeting this employer market specifically for in-home care solutions.
To position for risk-bearing contracts in years 3 to 5, you need data infrastructure now. Start collecting outcomes data, cost data, and patient experience data from day one. Value-based contracts require you to prove your intervention changes total cost of care—not just that patients like your service.
Decision Framework for Health Tech Boards
If you’re a founder presenting hospital-at-home strategy to your board, or a board member evaluating your company’s approach, here are the right questions to ask.
5 questions your board should ask right now
What percentage of our revenue depends on waiver-specific reimbursement? If it’s above 50%, you have concentration risk. Diversify your payer mix and care settings.
If the waiver expires in 5 years, what’s our Plan B business model? You should have a concrete answer. Can you pivot to post-acute care? Palliative care? Chronic disease management? If the answer is “we’re screwed without waivers,” you’re not building a durable company.
Are we building technology that creates value in multiple care settings? The best health tech platforms work across hospital-at-home, skilled nursing, home health, and ambulatory settings. Flexibility equals durability.
How quickly can we prove margin-positive unit economics? If you can’t show positive contribution margin by month 24, extending the timeline to month 36 won’t magically fix the problem. You have a business model issue, not a scale issue.
What’s our competitive moat if 10 other startups get this same 5-year runway? Policy tailwinds create competition. What’s your defensible advantage? Clinical outcomes data? Payer relationships? Technology that’s genuinely better, not just first to market?
Investor perspective on policy-dependent businesses
Source: WallStreetMojo
VCs underwrite regulatory risk by discounting valuations and requiring faster paths to profitability. A pure software company might get 7-10 years to reach profitability. A health tech company with policy dependency gets 3-5 years maximum.
Some investors love policy tailwinds. They want to ride the wave while it’s building. Others avoid policy-dependent businesses entirely, no matter how attractive the market opportunity looks.
Position your pitch carefully. Are you policy-enabled (taking advantage of favorable reimbursement to scale faster) or policy-dependent (can’t exist without specific waivers)? The former gets funded at reasonable valuations. The latter struggles.
What I Wish Existed When I Was a Caregiver
Let me bring this back to why any of this matters. The technology decisions health tech founders make over the next 24 months will determine what tools families like mine have access to in 2026 and beyond.
The gap between technology capability and real-world reliability
Source: Aptiva Medical
My husband’s Dexcom continuous glucose monitor worked beautifully—when it synced properly. The app sent alerts to my phone whenever his blood sugar went dangerously high or low. That device probably saved his life multiple times.
But it only worked because the technology was reliable:
The sensor stayed attached.
The Bluetooth connection held.
The app didn’t crash.
I’ve seen hospital-at-home platforms that look impressive in demos but break under real caregiver stress. The dashboard shows beautiful data visualizations—but requires three different logins to access. The monitoring devices pair easily in the clinic—but fail when WiFi is weak in rural areas.
Care coordination platforms often assume 24/7 nurse availability. They don’t account for the reality that small hospital-at-home programs can’t staff round-the-clock coverage.
Build for the worst-case scenario, not the ideal one.
Building for the sandwich generation managing multiple conditions
Source: Graying with Grace
My husband had 10 doctors. Ten! A primary care physician, nephrologist, endocrinologist, oncologist, cardiologist, and five other specialists. Your platform needs the capability to handle that complexity.
Nobody coordinated between them. I was the coordination layer. I maintained a spreadsheet with all his medications—drug names, dosages, prescribing doctors, reasons for taking them, refill schedules. The nurses loved my spreadsheet because their systems couldn’t give them the same view.
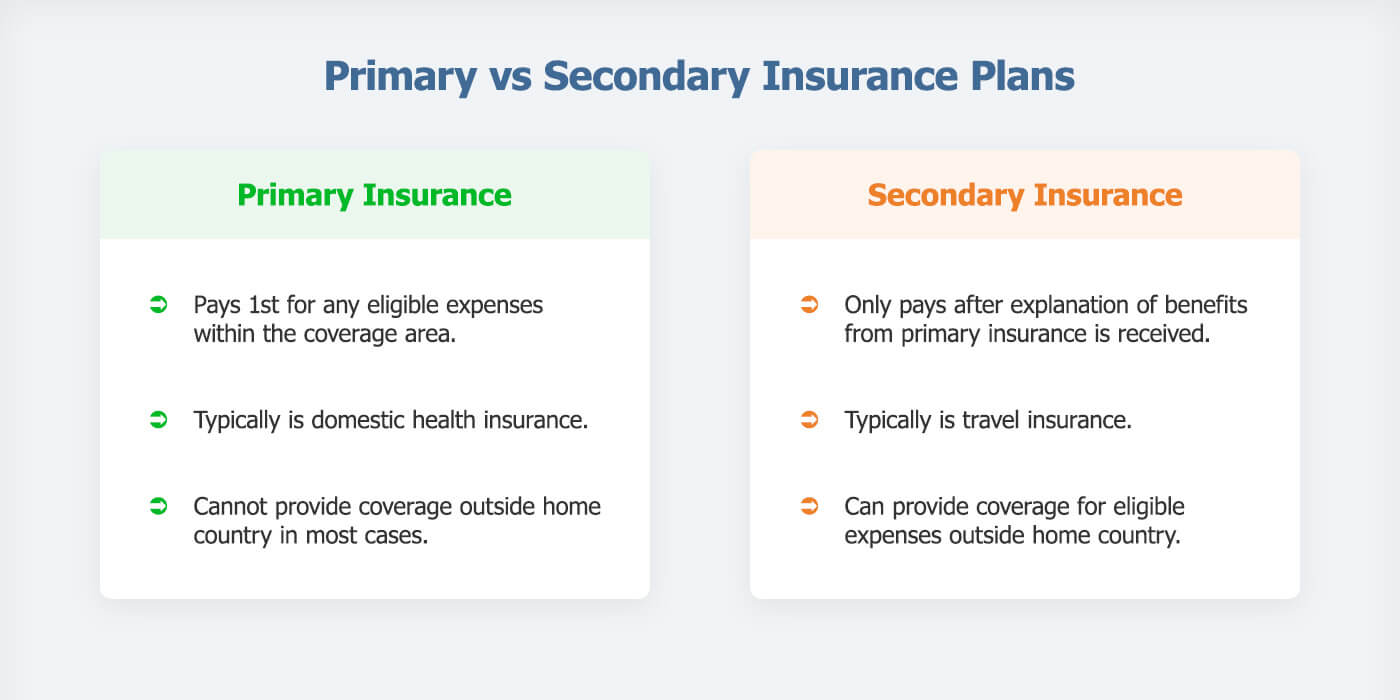
Insurance coordination created endless frustration. My employer’s insurance was primary while Medicare was secondary. Every billing department called me multiple times to confirm this. I explained the same thing to the hospital billing office, the lab, the imaging center, the pharmacy.
Your hospital-at-home platform should automate this nightmare. Pull medication lists from multiple prescribers. Flag potential drug interactions. Coordinate insurance claims automatically. Don’t make family caregivers become project managers.
Why I care about this 5-year window
Families like mine in 2026 deserve better than what I had in 2016.
The technology exists now, and the clinical models work. The question is implementation and sustainability.
Health tech founders have a moral obligation beyond shareholder returns. Yes, you need to build a profitable business and generate returns for your investors. But you’re also building tools that will serve people during the most vulnerable moments of their lives.
This isn’t about making a quick buck off temporary Medicare waivers then exiting before they expire. It’s about building something that lasts. Something that works. Something that actually helps families manage impossible complexity.
When you’re making technology decisions over the next 24 months, remember: real people will rely on what you build. Build something worthy of that trust.
The Path Forward
The proposed 5-year extension for hospital-at-home waivers isn’t a guarantee. It’s a window.
What you build in the next 24 months determines whether your company survives beyond 2030—regardless of what happens with federal policy.
The smartest founders build technology that creates value across multiple reimbursement scenarios. Focus on margin-positive unit economics. Solve real problems for real families—the kind of problems I faced as a caregiver managing impossible complexity across disconnected systems.
Start with the unsexy AI that makes programs profitable: revenue cycle management, clinical documentation, coding accuracy. These aren’t sexy pitch deck slides, but they generate cash flow.
Build your minimum viable stack around care orchestration and monitoring that works when human resources are constrained. Health systems can’t hire infinite nurses. Your technology needs to make existing staff dramatically more productive.
Structure pilot programs that generate defensible ROI data within 6 months. You need proof points for your next fundraise and for health system expansion.
Stress-test your business model. If hospital-at-home waivers expire in 2030, what’s Plan B? If you don’t have a good answer, you’re building on quicksand.
Five years is enough time to build something durable if you start with the right foundation. It’s not nearly enough time if you’re building for a policy moment instead of a market need.
The families who need hospital-at-home can’t wait for perfect policy clarity. They need technology that works today and keeps working tomorrow. So build for that reality.
Want to discuss your hospital-at-home technology strategy?Connect with me on LinkedIn or explore more health tech analysis at reewrites.com.
References
Bessemer Venture Partners. (2026). State of Health AI 2026. Retrieved from https://www.bvp.com/atlas/state-of-health-ai-2026
Fox, A. (2026). 2026 House spending bill proposes 2-year telehealth and 5-year hospital-at-home waiver extensions. Healthcare IT News. Retrieved from https://www.healthcareitnews.com/news/2026-house-spending-bill-proposes-2-year-telehealth-and-5-year-hospital-home-waiver-extensions
Gardner, S. & Hooper, K. (2026). Health tech panel to reboot after a long break. Politico Pulse. Retrieved from https://www.politico.com/newsletters/politico-pulse/2026/01/21/health-tech-panel-to-reboot-after-a-long-break-00737790
Gonzales, M. (2026). Proposed Funding Package Would Extend Hospital-at-Home Program, Medicare Telehealth Flexibilities. Home Health Care News. Retrieved from https://homehealthcarenews.com/2026/01/proposed-funding-package-would-extend-hospital-at-home-program-medicare-telehealth-flexibilities/
Stock Titan. (2026). Cubby secures $63 million in Series A funding round led by Growth. Retrieved from https://www.stocktitan.net/news/GS/cubby-secures-63-million-in-series-a-funding-round-led-by-growth-ikgye2ab40md.html
Zanchi, M. G. (2026). AI Journal. The “unsexy” revolution within healthcare AI. Retrieved from https://aijourn.com/the-unsexy-revolution-within-healthcare-ai/
I went to the CES 2026’s Digital Health Summit in my new city of Las Vegas, and yes, I oohed and ahhed at the dancing robots and awesome cars and vehicles on display.
But this isn’t your usual “look at this shiny new device” content you’ll see everywhere else about CES. I’m going to share the hard truths that came directly from patients, caregivers, and the organizations who represent them.
Left to right: Jennifer Goldsack, Randall Rutta, Alice Pomponio, Jake Heller, and Yuge Xiao
Product Design Failures Nobody Talks About
Your product design isn’t neutral
Randy Rutta from The National Health Council shared a couple of stories that should make every product team pause:
A major pharma company launched inhalable insulin with all the confidence in the world. The technology was solid, and the marketing was ready, but it flopped completely because they never asked patients if they’d actually use it.
It turns out that people managing diabetes need precision. Something sprayed into your lungs doesn’t feel precise, even if the science says it is. Plus, patients hated the inhaler design itself. Simple focus groups made of their target user base would have caught both issues before millions were spent on development and launch.
Another story hit even harder for me as a Black woman. Randy said a Black woman refused to wear a health monitoring device because it was a bulky black device on her waistband that made her afraid of being stopped by police. Her solution was painfully simple: “If it came in pink, it would have changed everything for me.”
This isn’t about inclusion for inclusion’s sake. It’s about building products that don’t put users at risk. Product design is literally life-or-death for some users.
Randy also mentioned patients with eczema and psoriasis who can’t wear certain devices because they’re too sensitive to materials touching their skin. That’s a deal-breaker for entire patient populations—a product design consideration that could eliminate your addressable market if you ignore it.
Engage patients early or pay later
Alice Pomponio from American Cancer Society’s venture capital arm sees this pattern constantly. You have to think beyond product features to systemic change. She asks founders: “What is not only the short-term product development strategy, but also the longer-term healthcare systemic step change you’re planning to deliver?”
Get patient voices around your cap table. Diversify your board perspective. Even if you have a great management team with good intentions, without a board that supports patient-centered decisions, you’ll lose the opportunity to make cost-effective strategic choices upfront.
It’s cheaper to fix problems during design than during M&A negotiations when your product strategy determines your acquisition price.
Women’s Health Tech Is Broken
Left to right: Sheena Franklin and Maya Friedman
Women are done waiting for tech that works for THEM
Sheena Franklin of K’ept Health interviewed Maya Friedman from Tidepool about how healthtech uses males as the default for AI.
Maya dropped a statistic that should embarrass the entire diabetes tech industry: 70% of women with type 1 diabetes experience insulin sensitivity changes around their menstrual cycles,but there are NO clinical guidelines or algorithms designed for this. Nothing. So women have to manually adjust their diabetes management systems every single month because the technology assumes their bodies work like men’s bodies.
“We need to stop thinking about women’s health as reproductive health. 𝘌𝘷𝘦𝘳𝘺 𝘴𝘪𝘯𝘨𝘭𝘦 𝘩𝘦𝘢𝘭𝘵𝘩𝘤𝘢𝘳𝘦 𝘤𝘰𝘮𝘱𝘢𝘯𝘺 𝘯𝘦𝘦𝘥𝘴 𝘪𝘯𝘧𝘳𝘢𝘴𝘵𝘳𝘶𝘤𝘵𝘶𝘳𝘦 𝘧𝘰𝘳 𝘥𝘢𝘵𝘢 𝘤𝘰𝘭𝘭𝘦𝘤𝘵𝘪𝘰𝘯 𝘢𝘵 𝘵𝘩𝘦 𝘪𝘯𝘵𝘦𝘳𝘴𝘦𝘤𝘵𝘪𝘰𝘯 𝘰𝘧 𝘸𝘰𝘮𝘦𝘯’𝘴 𝘩𝘦𝘢𝘭𝘵𝘩.”
The data gap is massive
Maya Friedman
Maya referenced a project called “The Library of Missing Data Sets,” an art exhibition of hundreds of empty filing cabinets labeled with data sets that don’t exist across different industries. When you look at what’s missing, you see where biases already exist in healthcare.
As AI becomes more prevalent, these data gaps will replicate the same biases we’re trying to fix. That’s why every healthcare technology company needs infrastructure for data collection at the intersection of women’s health. Not as a “nice to have.” As a business requirement.
Tidepool partnered with Oura to build the largest longitudinal data set of diabetes device data combined with biometric data. They’re distributing Oura rings to thousands of users already on the Tidepool platform. The data will include:
Activity tracking
Sleep patterns
Menstrual cycle data
Diabetes device data from the same individuals
Health surveys for contextual data
This is what infrastructure looks like when you take women’s health seriously.
Algorithms need to be smarter
Maya’s immediate priority: building algorithms that aren’t “cycle agnostic.” She wants systems that account for 30-day hormonal patterns, not just 72-hour learning horizons.
“Women are not just tiny men. We have different needs. We need to display different data. We need algorithms that are potentially different for women versus men.” – Maya Friedman, Tidepool
And yes, that means maintaining multiple versions of products.
Yes, it’s more expensive. But it’s also addressing the actual market need instead of pretending half the population doesn’t exist.
It’s not just about menstrual cycles
Maya’s longer-term vision includes AI models that are dynamic across different reproductive milestones. What does an algorithm look like for someone in perimenopause who isn’t having regular periods? What are the learning horizons for that system?
The real moonshot? A fully closed-loop system that accounts for polycystic ovarian syndrome (PCOS), type 1 diabetes, and menstrual cycles without requiring patient interaction at all.
Women need tech that doesn’t make them choose between their health needs and their time.
Accessibility Creates Market Opportunities, Not Limitations
Left to right: Steve Ewell and Peter Kaldes
Peter Kaldes, CEO of Next50 Foundation, delivered a message that should change how every product designer thinks about their addressable market: “Guess what? You still have a point of view over 50. You still have buying power at 60. You can still use your iPhone at 70, and you need really great technology in the 80s and your 90s.”
Most product designers are under 35. Most assume older adults are technology Luddites. The data proves this assumption is completely wrong.
The buying power is enormous
The over-50 population has more buying power than younger generations. Yet, healthtech companies consistently ignore this market or, worse, design products that stigmatize older users. Peter’s frustration was that was crystal-clear:
“I’ve had conversations with some companies like, where are we going to find [older users to test with]? Well, why don’t you try, first of all, start with your company, and second of all, why don’t you start partnering with community organizations that have access to all these people. This is not hard. It’s just getting people out of their comfort zone.” – Peter Kaldes
Dual generational use is smart design
Peter loves technologies that serve multiple generations. If it’s good for older adults, it’s good for everyone. Examples he highlighted:
Hearing technology embedded in glasses to reduce stigma around hearing aids
AI tools that coordinate healthcare appointments along with transportation and nearby housing options
Financial fraud protection that helps older adults without treating them like children
Left to right: Meg Barron, Dominic King and Myechia Minter-Jordan
AARP CEO Myechia Minter-Jordan shared specific examples of products in AARP’s booth that reduce stigma:
Sneakers designed to prevent falls that look like regular athletic shoes (they appear to have laces, though velcro is involved)
Glasses with closed captions for people with hearing impairments
Glasses with hearing aids built into the stems (partnered with Sadika)
“We want to ensure tools don’t further stigmatize us but allow us to live with dignity and age well.” – Myechia Minter-Jordan
The accessibility-to-mainstream pipeline
Left to right: Natalie Zundel, Griffen Stapp, Ryan Easterly and Jack Walters
Griffen Stapp from Ability Central pointed out something product teams consistently miss: Products designed FOR the disability community often get adopted by everyone. But products made for the general population rarely get adapted later.
Examples are everywhere. Curb cuts help wheelchair users, but they also help parents with strollers, delivery workers with hand trucks, and travelers with rolling luggage. Closed captioning helps deaf users, but also people watching videos in noisy environments or practicing language skills.
Build accessibility in from day one, or you’re leaving both impact and revenue on the table.
Adaptable frameworks beat one-size-fits-all
Jack Walters, co-founder of HapWare (winner of the CTA Foundation Innovation Challenge), explained their approach: “Not everyone’s going to have similar care or similar treatments, so you need to be able to adapt to all those different types of needs and necessities in the community.”
They involve the disability community in design from the start, knowing common pain points and anticipating when certain issues might come up. That’s how you build solutions that actually solve problems instead of creating new friction.
Continuous Monitoring Changes Patient Behavior (Without Doctor Visits)
Left to right: Ami Bhatt, Tom Hale, Lucienne Ide and Jack Leach
Tom Hale, CEO of Oura, explained why continuous data matters more than episodic measurements: “Normal isn’t 98.6 degrees. Normal is what’s normal for you, and being able to see that deviation from the baseline allows us to make predictions.”
Oura’s “symptom radar” looks at temperature, heart rate, and other biometrics to predict when you might be getting sick—days before symptoms appear. That’s the intervention window where you can actually change behavior and potentially avoid getting sick entirely.
Patients change behavior when they see their own data
Jake Leach from Dexcom shared a pivotal study from the early days of continuous glucose monitoring. For years, the standard of care for diabetes was finger pricks, which are episodic, painful, and limited.
They ran a study where they put sensors on patients continuously measuring glucose, but they didn’t show patients the data for a week. They just collected baseline information. Then they turned on the display.
Within a day, people started making behavior changes based solely on their own knowledge of their disease and this information they’d never had before. No doctor intervention. No coaching. Just visibility into their own patterns.
The infrastructure problem doctors face
Source:Somebody Digital
Doctors are drowning in data with no infrastructure to process it.
Lucienne Ide from Rimidi left clinical medicine because she was disappointed by how electronic health records (EHRs) were implemented. She expected digital records with clinical decision support layered on top. Instead, she got data dumps with no insights.
As she put it: “I don’t know a single doctor who’s saying, ‘If only I had more data, I would be a better clinician.'”
What doctors need is not more data, but clinical decision support that turns data into actionable insights.
Tom from Oura said one doctor told him: “I want the Oura ring to give me information as if it was written by another doctor. Basically, a consult. Here’s what I know about this patient in clinical terms, and this is the information you need. Everything else, don’t give it to me.”
That’s the responsibility of device companies: Don’t just collect data. Provide insights that save clinicians time and help them make better decisions faster.
Prevention requires behavior change at scale
The consensus was clear: behavior change is what moves the needle on long-term health outcomes. Not medications or procedures. Sleep well, eat well, manage stress, and stay balanced.
Healthcare has failed at behavior change for 75 years because it requires data, user experience (UX), engagement, education, and reinforcement. Doctors don’t have time for that level of ongoing support. Educational content alone doesn’t work because people don’t retain or apply it without reinforcement.
But continuous monitoring combined with AI and smartphone engagement is the combination that finally makes prevention scalable.
As Ami Bhatt from the American College of Cardiology noted, “What has my attention besides my kids? My phone. And I’m looking at that, and that’s the power.”
AI That Actually Helps, Not Hypes
Source:Oxio Health
Dominic King from Microsoft AI cut through all the conference noise:
“The biggest challenge in healthcare today is the mismatch between global demand and constrained supply.” – Dominic King
AI isn’t replacing doctors. It’s closing the gap between what people need and what the healthcare system can deliver.
The future is proactive health companions
5 years ago, AI was good at classification and spotting single problems. Now we have thinking and reasoning models that can pass the same exams physicians take, often at higher rates than human test-takers.
Dominic’s vision for 5 years from now is “A health companion that you wake up and it’s sitting in the background, doing the hard work for you and being more proactive. At the moment, everything is still very reactive.”
This means:
Identifying sleep issues before they compound
Flagging medication adherence problems
Coordinating complex care across multiple providers
Helping people navigate fragmented healthcare systems
Providing specialized opinions even in rural areas
The caregiver opportunity is massive
Myechia shared that one in four Americans are caregivers right now (63 million Americans). If you’re not currently a caregiver or need care yourself, one day you will be.
AI tools can help caregivers:
Communicate with provider teams more effectively
Ensure loved ones are safe at home
Coordinate the “universe of appointments” that comes with aging
Reduce information asymmetry (where only people with medical training understand how systems work)
Dominic emphasized that co-design is critically important. Building WITH users instead of just FOR them avoids the problems we see when products hit the real world.
At Microsoft, they’re seeing 50 to 60 million health questions a day through Copilot. That’s enormous insight into what people actually need help with.
But as he noted, “A lot of founders are young. They don’t have a good idea of what it’s like to be elderly or sick.”
That’s why bringing your end users (patients, clinicians, caregivers) into the development process isn’t optional. It’s the difference between building something that works versus something that sits unused.
The Digital Equity Gap Nobody’s Solving
Left to right: Steve Ewell and Peter Kaldes
Steve Ewell, Executive Director of CTA Foundation, laid out what he calls “the three legs of the stool” for digital equity:
“You need the hardware, you need the broadband access, and then you need the support and education to go along with it. And so often that last one is left off.” – Steve Ewell
That last leg of support and education is where healthcare technology adoption actually lives or dies.
Tech alone isn’t enough
Peter Kaldes from Next50 Foundation added context that should worry anyone in healthtech: nonprofits doing the heavy lifting of digital equity training are facing unprecedented cuts to federal grants.
As Peter noted: “I love going to an Apple Store and seeing these free classes, but you have to find an Apple Store which are not in the neighborhoods that need the help the most.”
The communities that need technology training the most are the least likely to have access to it. And the organizations that bridge that gap are losing funding.
The clinical trial proof
Source: Anatomy.app
Dexcom is running large clinical trials where half the participants come from underserved communities specifically to prove the technology works equally well regardless of service level. They want hard data showing these tools aren’t just for people with resources.
Rimidi partnered with community health centers during COVID to monitor high-risk pregnancies remotely using blood pressure monitors and texting protocols. They tracked engagement by ethnicity and primary language.
There was no difference in engagement. Everyone has a smartphone in that demographic (women of childbearing age), and everyone can text.
This proves that engagement isn’t the problem. The problem is getting access to the infrastructure and training on how to use it.
Mission-aligned capital as the solution
Source: Next50 Foundation
Next50 Foundation is one of the first private foundations to invest 100% of their endowment in aging-focused companies and infrastructure. Not just grant-making, but the other 95% of their capital.
They created an aging investment framework with JP Morgan that looks at four themes:
Health
Social connectivity (including technology)
Economic opportunity (workforce and financial vehicles for longer lives)
Built environment (mobility, housing, accessibility)
As of December, about 75% of their endowment was invested in this framework, and Peter offered a challenge to the investment community:
“What if capital actually had values? Climate investors have successfully made money and helped power cleaner energy. The same can be true for aging. How can we possibly ignore that the globe is aging?” – Peter Kaldes
They also launched a new nonprofit called Leverage focused on advancing policies in Colorado to make aging more affordable—housing, living wages, caregiving resources.
Because you can’t solve systemic problems with technology alone. You need policy change too.
Patient Voices Need to Drive Startup Decisions
Jake Heller from Citizen Health is building AI tools that help patients with rare diseases query their own medical records and advocate for themselves at doctor’s appointments.
His philosophy: “Putting patients in the driver’s seat is one of the biggest opportunities we have right now.”
The journaling and documentation problem
Sometimes when people with rare or complex diseases go to appointments and talk about their concerns, doctors don’t believe them. These patients need help translating their own experience in a way that clinicians will take seriously.
Citizen Health helps patients journal their symptoms and experiences, then presents that data in clinical terms. “Here’s a video of my daughter having this specific type of seizure. Here are the journal entries. Here’s how this has changed over time.”
That’s advocacy powered by data and AI.
The time-to-diagnosis crisis
Randy pointed out that if you have an autoimmune disease, it could be 3, 5, or even 7 years before diagnosis. For healthcare innovation, it can take 7 years just to move something through an FDA process.
Those time frames compound into suffering that’s completely preventable if we had better systems and patient input earlier in development cycles.
Patient organizations are ready to help. They’re trusted by their communities. They can broker relationships, speed recruitment, help startups get from lab to market faster with products that patients will actually use and that payers will actually reimburse.
The startup trap to avoid
Source: National Institute for Health and Care Research (NIHR)
Alice warned about companies that design products, then go looking for users to validate decisions they already made.
That’s backwards. Instead you should:
Find patient voices early.
Put them on advisory boards.
Include them in design sprints.
Listen to their feedback even when it’s uncomfortable or expensive to implement.
The successful companies in her portfolio think about long-term systemic change, not just short-term product development metrics.
What Healthtech Companies Need to Do Differently
The patient community isn’t a barrier to innovation. They’re the key to building products that actually work.
Stop designing in the dark
Source: Patient Better
If you’re building healthtech without continuous patient input, you’re wasting resources. You’ll miss market opportunities. You’ll build products that don’t get used or that put certain populations at risk.
Randy’s message was clear: “Come to us, and we will broker that relationship, because in the end, you’ll be more successful, and the patient community will get a better result.”
Measure what matters
Myechia challenged the AI industry on how they measure success: Don’t count the number of tools or features. Measure whether you’re closing the gap between lifespan and health span.
That gap is currently 13 years, which is the difference between how long people live and how many of those years are healthy years. If your technology doesn’t move that number, what’s the point?
Think systemically, not just tactically
Source: IQ Eye
Every speaker emphasized that technology is only one piece of a larger puzzle. You also need:
Policy changes that support adoption
Payment models that reward prevention
Training infrastructure for underserved communities
Clinical decision support that turns data into insights
Algorithms that account for biological differences across populations
If you’re only focused on your device or platform, you’re missing the bigger picture of how healthcare actually works.
The sales enablement angle
All of these insights about patient needs, accessibility requirements, women’s health gaps, digital equity challenges are the stories your prospects need to hear during long sales cycles.
B2B healthtech sales aren’t quick. You’re selling to health systems, payers, and large provider networks. The buying committees are complex. The evaluation periods stretch for months.
That’s exactly when prospects go cold or arrive at sales calls unprepared.
I create educational email courses to bridge that gap. They keep prospects engaged with the exact kind of patient-centered insights I heard at CES. They position your company as one that understands real-world healthcare challenges, not just technology features.
In 2026 and beyond, healthtech companies that want to win understand their users deeply enough to build products those users will actually want, trust, and use.
The Measurement Challenge
How do you know if you’re succeeding at patient-centered design? Myechia offered a simple test: “What do you want your life to look like at 75?”
You probably want to:
Stay in your home
Feel healthy
Stay empowered
Have information flow easily between you and loved ones
Remain connected to family and physicians
Be safe at home
Engage in daily activities with ease and without pain
Understand your medical information and chronic diseases
Control who has access to your data
Have a care plan you can execute yourself
Receive information you trust and can use readily
If your tech helps people achieve any of those goals, you’re on the right track. If it doesn’t, you need to rethink your approach.
Final Thoughts
CES 2026’s Digital Health Summit covered the hard work of actually listening to patients, caregivers, and the communities being served.
Startups who want to be successful in healthtech aren’t the ones chasing the next funding round or the flashiest AI feature. They’re the ones asking better questions:
Have we talked to patients who look different from our team?
Does our product work for women’s bodies, not just male bodies?
Can older adults use this without feeling stigmatized?
What infrastructure needs to exist beyond our technology?
Are we solving a real problem or just building something technically impressive?
Those questions lead to products that get adopted, outcomes that improve, and companies that actually make a difference. That’s the kind of healthtech worth building.
The intersection of chronic illness management and in-home caregiving presents unique challenges in healthcare. Through a compelling blend of personal storytelling and empirical data, this article illuminates the often-overlooked daily struggles of working caregivers.
I examine how emerging technologies and care models such as remote patient monitoring and care-at-home programs can transform the caregiving experience, offering valuable perspectives for healthcare providers and health plans seeking to integrate effective care solutions.
I married a man just two months after we met, because if I didn’t, I knew he was going to die.
I met George on a dating site in March 2016 as “PuertoRicanPapi.” During our first phone conversation, I learned he had been diagnosed with Stage 4 end-stage renal disease (ESRD) and only had 18 months to live. He needed to start dialysis, but his ACA health plan wouldn’t cover it.
The Global Burden of Disease ranks chronic kidney disease (CKD) among the top 20 causes of death (Ibrahim et al., 2022). CKD is regarded as a high-stress illness due to the chronicity of the disease and the long-term treatment required. ESRD is the last stage of CKD, often caused by diabetes mellitus.
That’s a heavy thing to hear from anyone. But there was something about him that wouldn’t let me leave him alone.
The Downward Spiral
The Diabetes Domino Effect
George was a 40-year-old Puerto Rican man with diabetes, neuropathy, and ESRD. The following year, he developed non-Hodgkins lymphoma (NHL) and eventually sepsis. Over the course of our 2 years together, I coordinated his care among 10 doctors (primary care and various specialists).
His diabetes diagnosis is unclear, as some of his doctors mentioned Type 1 and others said it was Type 2. But from what I understand, before we met, a clinic had prescribed him insulin pills when he actually needed the insulin pens.
That’s a heavy thing to hear from anyone. But there was something about him that wouldn’t let me leave him alone.
Peritoneal Dialysis and the Hospital Revolving Door
That fall, George got surgery to implant a port into his belly, and then we started peritoneal dialysis (PD) from home. I set up the machine and ran it for him every night as I was taught by his nephrology team. But every month he went to the hospital because:
A1C was high,
His hemoglobin count was low (especially after chemotherapy) and he needed a blood transfusion, or
He was in pain.
He didn’t like being there because no one would let him rest, nutritionists came in to tell him how to eat properly for a diabetic and renal diet (and often those menus were contradictory), and other clinicians would come in and ask the same questions every time. I occasionally stayed overnight with him if my daughter was accounted for.
Weekends were the worst, because when he was having intense pain, he had to visit the ER for relief, of course waiting all day for his name to be called.
We also enrolled in a kidney transplant program at Emory Hospital in Atlanta, GA. Although I wasn’t a match to be a kidney donor for George, I was eligible to be in an exchange program with someone else, and they could provide a matching kidney for George. Unfortunately, the next setback negated these efforts.
Developing Cancer
George saw the dentist for pain in his mouth a few times in the fall of 2016 and spring of 2017. The dentist found an abnormality in his mouth that kept coming back.
During that last visit, George went to the hospital, they tested it and it was cancer–Non-Hodgkins Lymphoma (NHL).
He started chemotherapy later that month. His beautiful hair started shedding on the pillowcase the next day, and mourning began.
Losing his Leg
A few months later, George fell in our bathroom upstairs while I was in New York at my grandmother’s funeral. His teenage daughter was home, but downstairs. She called me two days later to tell me that he fell, and that his foot was black.
Source: Alltech Prosthetics
Type 2 diabetes often causes complications that can lead to lower limb amputation (Costa et al., 2020), and unfortunately, this is when George’s health took a turn for the worse. We went to a specialist after I got back from New York, who confirmed his left foot was broken and would probably never heal correctly, and recommended a below-the-knee amputation. George was devastated, but went through with it.
Afterward, he could still drive with his right foot, and he decided to buy a large SUV. I assisted him with getting in and out of the truck with his new wheelchair. However, we no longer slept together, because our bedroom was upstairs. He stayed on the couch for a few months until we got a hospital bed placed in the living room.
Losing Hope
Even though he was taking several prescribed high-dose narcotics, they didn’t have much effect in pill or patch form. Only medicines administered by IV quelled his suffering.
I always felt like I had to be strong, but I was at my wits end, suffering silently beside him. The last straw was when he developed gangrene on his genitalia, and it wasn’t curable. His pain intensified, and I advocated for him tirelessly by calling doctors, and researching information, but it was impossible to get pain management from any doctor in our city, so he suffered needlessly.
Multiple calls to his nephrologist and primary care doctor were never addressed, so I believed that palliative care was the only thing that would make him comfortable. In January 2018, I admitted him to hospice care, where he died a couple months later. I didn’t receive follow-up counseling afterward, but I met with my therapist a few more times until I moved out of state and back near my family to grieve.
Looking Back
The single most important thing missing from my experience that would have made things easier is access to support, which I describe in the following DECAF section.
I balanced parenting and school functions with spousal caregiving, administrative duties like tracking his medications, scheduling new appointments and conferring with health insurers, transporting my husband to multiple appointments, household responsibilities, and my full-time work as a technical writer with a Fortune 50 corporation. And I didn’t receive support from providers after his death, except for a newsletter from the hospice team every few months until a year passed.
I could have used an assistant for appointment scheduling and insurance coordination. A home health aide at flexible times to help with toileting and other ADL tasks.
Effects of In-Home Caregiving by Working Adults
During the pandemic, parents of school-aged children learned what it’s like to try balancing the role of teaching them while also managing their own work and household responsibilities. In-home caregiving was similar in my experience-–I had to juggle my work duties working from home with caring for my husband, and it wasn’t easy.
A study of the estimated 8.8 million employed family caregivers found that nearly 1 in 4 (23.3%) reported either absenteeism or presenteeism over a 1-month period due to caregiving (Fayete et al., 2023). Among those affected, caregiving reduced work productivity by one-third on average—or an estimated $5,600 per employee when annualized across all employed caregivers—primarily because of reduced performance while present at work. Productivity loss was higher among caregivers of older adults with significant care needs and varied according to sociodemographic characteristics and caregiver supports.
CareYaya Health Technologies’ data shows that caregivers spend an average of 15 to 20 hours per week on caregiving tasks. “It’s super hard to draw the line between when you’re working and when you’re caregiving when you’re WFH,” says CEO Neal K. Shah.
“70% of caregivers worldwide are women, and their average age is 49,” says Cheryl Field, MSN, RN. “So if you think about the multiple roles that a 49-year-old woman is playing between their own children, their career, their parents, their partner and the biological changes that come with menopause, you can see that caregivers are in a particularly pressure-filled time of their life. Any means by which they can reduce some of these stressors is significant.”
Stress from Multitasking
Source: Position is Everything
Caregiving influences several dimensions of the caregiver’s life, such as physical (e.g., physical health deterioration), psychological (e.g., anxiety and traumatic stress), family (e.g., roles and routines) and social (e.g., leisure time and social life) (Costa et al., 2020). Caregivers under stress report high levels of depressive symptoms, anxiety, high use of psychotropic drugs, low satisfaction with life, several symptoms related to psychological stress, and low subjective health.
“In-home caregiving lends itself to both more and less stress for the caregivers,” notes Dr. Caryn McAllister of High Quality Therapy. “Caregivers who work from home can juggle responsibilities needed during the day with work, and flexibility with respect to hours can allow people to contact medical professionals, organize schedules, and ensure their loved one eats, goes to the bathroom and takes medicines on time. The extra stress can come when people don’t have the ability to transition between work and home life. People often find they can leave work at work when they go home, but caregivers who work from home just don’t get that break. Ever! It takes organization and discipline to make it work.”
Wil Thomas, Editor of the Senior Bulletin, mentions a reader named John who echoes these sentiments. John has a full-time job while taking care of his elderly mother. “It’s like having two full-time jobs,” he says. “I’m constantly juggling meetings and her medical appointments, and it’s exhausting.”
Field understands this, too. As a former chief product officer who had a senior living with her in a multigenerational setting. She highlighted that the impact of providing in-home care varies over the course of the patient’s illness. “When care needs can be anticipated and scheduled, and additional resources can be utilized to put a plan in place, the impact can be smaller. When care needs are unexpected or difficult to anticipate, the impact will be greater,” she says.
“Consider that your interrupted sleep several times a week in the middle of the night over a chronic period of time begins to have an impact on your own rest and even the ability to fall asleep with anticipated anxiety of what’s to come through the night,” Fields continues. As care needs become more demanding on working adults, often you’ll see a rise in absenteeism for scheduled and unscheduled medical needs, and a decrease in resiliency on behalf of the employee. Chronic fatigue, fear, stress and anxiety all compound and can have an impact on the health of the working adult.”
Unfortunately, these stories aren’t unique. For adults who are caring for a loved one and also continuing to work in their career, taking on these responsibilities can be stressful and lead to burnout, Field says. 60% of caregivers are also employed, and many feel the job-related stress piling up. But working from home does make a big difference, providing flexibility that in-home caregivers need.
Impact of Diabetes on Patients and Chronic Care
50% to 75% of people with diabetes have a caregiver involved in their healthcare (Fields et al., 2022). These caregivers are often partners, spouses, adult children, or siblings.
Like many chronic conditions, diabetes requires complex medical management that often requires following regimented eating plans, monitoring sugar levels, organizing daily medications, and coordinating medical care. The sicker George became, the more of these responsibilities fell on me.
Source: eClinicalWorks
The chronic care model is a multidimensional solution to the complex problem of providing care to patients with chronic health problems. The theory of this model says that a significant part of chronic care takes place outside of formal healthcare facilities (Katsarou et al., 2023).
It also states that six elements are central to initiatives to improve chronic care: community resources, healthcare system, patient self-management, decision support, service delivery system redesign, and clinical information systems. Interventions that include at least one of these elements are associated with improved outcomes for people with asthma, diabetes, heart failure, and depression. However, only patients with heart failure and depression had improved quality of life (Katsarou et al., 2023).
Flexible scheduling
Caregiving would have been impossible if I couldn’t work from home. George had 10 doctors, and that translated to roughly 3 days a week with at least one appointment. At that point, I had worked for my company for almost 20 years, which gave me unlimited sick time and lots of vacation time. I took my work laptop with me to doctor appointments, rearranged meetings, and still made time for my daughter’s activities.
Working from home gave me flexibility in managing caregiving tasks and professional responsibilities, including the ability to respond to his needs promptly, compared to me working in an office setting, or George being in a facility where staff are spread across multiple patients.
Another of Thomas’ readers, Jane, works remotely and looks after her father, who has Alzheimer’s. “Working from home has been a lifesaver,” she says. “I can attend to my dad’s needs throughout the day without compromising my work. It’s still challenging, but having that flexibility makes a huge difference.”
While working from home offers more flexibility to manage caregiving tasks, it can also blur the lines between work and caregiving responsibilities. “Many caregivers report feeling constantly “on-call,” which can lead to burnout, and that burnout affects over 33% of family caregivers who are working from home, compared to 20% who work in the office,” Shah reports.
Indeed, flexible work arrangements such as telecommuting, job-sharing, and flexible hours can help caregivers manage their time more effectively. However, since the pandemic ended, return-to-office mandates have flourished with employers who want to manage employees in person and/or fill their empty office spaces. 90% of companies plan to implement return-to-office policies by the end of 2024, according to a report from Resume Builder. Nearly 30% say their company will threaten to fire employees who don’t comply with in-office requirements.
Source: SuperStaff
But for employees who can work remotely, several caregiver pressures can be relieved. Removing the commute and a strict start or end time of an office job gives the remote employee flexibility. Fields gives some of examples:
“On mornings where there’s been a difficult night, an extra hour of sleep can make a world of difference on how the employee feels and functions that day. Being able to work from home may also make it possible to leverage telehealth appointments instead of having to physically travel to doctor’s appointments. Caregivers also have the ability to provide distant supervision and mealtime support for a loved one while working from home and don’t need to have as many outside resources coming into the home to provide that supervision or ensure meals are delivered and consumed. These small benefits relieve a lot of microstress.”
Caregiver Needs Analyzed with DECAF
A study at the University of West Attica in Greece investigated the needs of caregivers of patients suffering from CKD, stroke, cancer, dementia and multiple sclerosis (Katsarou et al., 2023). 89% of these caregivers were relatives, 50% were between 20 and 50 years old, and 19% were spouses. Researchers found themes among caregiver needs:
Caregiver training
Help with nursing home care and physical therapy
Help with financial burden from health services
Lack of reliable transport
Psychological support, including delivery via digital media and mobile devices
Social support groups
Navigating complex medical insurance
I agree with all of these points. To break it down a bit more, I’m using the DECAF framework (Fields et al., 2022), which was developed to raise awareness about caregiver responsibilities in care planning and execution during the hospital-to-home transition. Here’s how DECAF played out in my caregiving experience.
Direct Care Provision
Direct Care Provision refers to hands-on support with activities of daily living (ADLs) such as getting dressed, food preparation, toileting and physical activities, and taking the patient to healthcare appointments. It also includes nursing tasks like wound care and medication management. I was a certified nursing assistant in the 90s, and a home health aide in the 2000’s, both of which prepared me for my experience with George.
Emotional Support
Emotional Support is the empathy and compassion for the patient and caregiver.
I had no close friends nearby, and George’s family was local, but most of them were more hands-off. So as his condition took more and more of a toll on my mental health, I sought out family members, a therapist, and church groups for support and stress relief.
Social support can diminish the impact of the emotional burden and stress of care by providing solutions to problems, distractions from issues or facilitating the required healthy behaviors (Ibrahim et al., 2022). Caregivers who seek social support from family and friends experience a lesser burden of care than caregivers without solid support networks.
Seeking social support is the dominant coping mechanism for caregivers of patients undergoing renal replacement therapy (Ibrahim et al., 2022). Caregivers of chronic patients are four times more likely to be diagnosed with depression and three times more likely to seek help for anxiety issues than individuals who are not caregivers.
Being an in-home caregiver is lonely, and I lacked self-care. I’ve been working from home since 2005 so I was used to being alone, but caregiving for your spouse is a different kind of loneliness. I was losing my husband slowly as his condition got worse, and I needed social support. I mostly relied on my family (long-distance phone calls) and a local church group. In less than a year, I shifted from being a newlywed with an independent husband to a caregiver. My marital needs were not met, as George lost sexual function early on. This also caused strain on our relationship.
I’m not alone. A study on psychological health from Savitribai Phule Pune University in India confirms that dysfunctions caused by chronic illnesses aren’t limited to the patient, but affect the partner, and the couple’s dynamic, making a considerable impact on the satisfaction levels in the relationship (Umrigar and Mhaske, 2022). Behavioral and personality changes in the patient can overpower emotional bonds between the caregiver and the patient as well. The greater the negative effect, the greater the frequency of depression, anxiety, and somatization in the caregiver.
This study polled women caregivers about their male spouses with chronic conditions of cancer, coronary heart disease, and diabetes. They found clinically significant marital and sexual dissatisfaction. Since marital satisfaction and sexual satisfaction are closely linked, a decrease in one tends to have a serious impact on the other, and consequently, on the overall quality of life.
Care Coordination
Care Coordination involves initiating, managing and maintaining healthcare services and support. Managing diabetes successfully requires significant care organization and coordination of multiple types of interactions with the healthcare system. Participants in a study at the University of Wisconsin-Madison (Fields et al., 2022) frequently recognized caregiver roles in care organization, such as helping with tracking and scheduling appointments, taking notes before and during healthcare visits, and making lists of current medications.
I can concur. I took George to his appointments, acting as an administrative assistant and advocate. It was up to me to take notes, ask for what he needed, and verify or dispel inconsistent information (test results, guidance, data, etc.) between different doctors. I had a spreadsheet that the nurses loved, because it listed all the pertinent information about his medication names, amounts, prescribing doctor, reasons for taking them, etc.
Patient Advocacy
Advocacy is about empowering individuals to obtain resources. In the same Wisconsin study, several participants described experiences where the caregiver advocated on behalf of the patient when experiencing serious health complications linked to diabetes.
I was no different. As the months went on, George’s depression intensified into hopelessness and an “I don’t care anymore” attitude. So in addition to caregiving, I was also a fierce advocate for his mental health, trying to find resources to alleviate his chronic pain and help him feel more comfortable.
Financial Support
Financial support refers to help with planning and using financial resources. With rising home and institutional care costs and formal caregiver shortages, 66% of caregivers use their retirement and savings funds to pay for care (Genworth).
Source: Grants for Medical
Applying for Social Security disability payments was a huge challenge. One of the questions that caused a denial related to his unemployment status. He explained that his medications made him fall asleep intermittently and randomly, so he couldn’t work. They blamed his medication and denied his application two more times before he was finally approved. He then started receiving payments of about $700 per month.
George had no life insurance, and I didn’t receive any direct financial support until his last week of life. I wrote Facebook posts about his status while he was in hospice care, and many of my friends sent funds via PayPal and Cashapp to help me pay for the funeral.
Navigating Healthcare Systems and Insurance Complexities
Caregiving at home often leads to substantial financial strain due to the cost of medical supplies, home health aides, and necessary modifications to the home. Not to mention the daunting task of navigating health insurance complexities, from finding in-network healthcare providers, care coordination, and working with billing offices regarding Medicare and Medicaid.
Finding In-Network Medical Providers
Another huge barrier for caregivers and patients alike is finding healthcare providers within their insurance network—especially specialists like those George needed. According to a Kaiser Family Foundation study, 29% of people struggle to find new providers within their network. Providers change the insurers they participate with frequently, and the onus is on the caregiver or patient to figure out how much of their bill will be covered in any given scenario.
Source: New York Bone & Joint Specialists
I’ve had to seek therapy before I met George, not just during his illness. No matter what, it’s difficult to find an available, local provider. Once I found a therapist, we started off going to see her together, but eventually he stopped.
Thomas recommends using online directories, insurance company tools and telehealth services to find these providers. And Dr. McAllister mentions an advanced step I’d never heard of before: “If you can’t find an in-network provider for your loved one, you can obtain a single case agreement, where your company will recognize the out-of-network provider as if they were in-network.”
Decoding the Difference Between Primary and Secondary Payer Insurance
One recurring source of frustration for me was dealing with multiple billing departments about George’s insurance. The health insurance from my employer was primary, and Medicare was secondary. I made this clear for each medical provider (remember, he had 10 doctors). However, each billing department would call me to confirm multiple times based on how his claims were processed.
Source: Drive Safe Insure
The coordination of benefits between private insurance and Medicare/Medicaid is something Shawn Plummer, CEO of The Annuity Expert educates his customers about. For example, he explains that determining the primary and secondary payers can help maximize coverage and minimize out-of-pocket expenses. Additionally, exploring supplemental insurance options can fill gaps not covered by primary insurance plans.
Healthcare providers have their struggles working with health insurance companies as well. Take for example Dr. McAllister’s practice, which is in-network with Medicare and out-of-network with all private insurance companies.
“As a provider, it’s so difficult to deal with insurance, although Medicare is very straightforward and easy to work with if you abide by their rules,” she says. “If you understand that private insurance companies try to maximize profit by denying coverage, and go into the process knowing how to advocate, you won’t feel as frustrated.
Source:: Geeks for Geeks
“To add to the confusion, when people have Managed Medicare, the medicare rules apply but the private insurance manages Medicare. “I often suggest sticking to straight Medicare, not Managed Medicare, because standard Medicare tends to treat providers more fairly. Many providers won’t accept Managed Medicare because of the low reimbursement rates and bureaucracy associated with private insurance companies.”
Bert Hofhuis of Sovereign Boss in the UK says that many insurance plans, including Medicare and private insurance, have limitations on what they cover for in-home care. “For example, Medicare may cover some home health services but often does not cover custodial care.”
Dr. McAllister, Hofhuis, and Plummer shared more tips to navigate complex insurance issues:
Source: Investors
Understand the specifics of health insurance policies: Ask questions about things you don’t understand, and “seek plans that cover in-home care services, medical supplies, and home modifications to be prepared,” says Hofhuis. “It’s essential to review policy details and consider supplemental insurance to cover gaps.”
Take notes: “When dealing with insurance representatives on the phone, always write down the name of the person you speak with, information regarding the call and a reference for the call. Write everything down and email as much as possible so you have proof of everything,” Dr. Allister says.
Use HSAs and FSAs: When available, Plummer and Hofhuis recommend usingHSAs and Flexible Savings Accounts (FSAs), which can provide tax-advantaged funds that can be used for medical expenses, including caregiving costs.
Plan for long-term care: Consider purchasing long-term care insurance early to cover potential future caregiving needs.
Keep records for tax purposes: Keep detailed records of caregiving expenses, as some may be tax-deductible, potentially easing your financial burden, Plummer and Hofhuis concur.
Denise M. Brown, is Founder and CEO of The Caregiving Years Training Academy, a family caregiving agency that coordinates care across multiple systems. She shares that Medicare Part B reimburses for Caregiver Training, Community Health Integration Services and Principal Navigation Services. Family caregivers can receive these services on behalf of a Medicare beneficiary if that beneficiary cannot participate in care planning because of their illness.
“The interplay between private insurance and Medicare/Medicaid is a common source of confusion,” Shah says. “More educational resources are desperately needed to help caregivers understand these complexities, including decision trees to determine primary and secondary payers.”
Effective Care Coordination Between Health Systems
Getting Access to Supplies and Services
The healthcare system is disconnected and siloed. The complications that come with coordinating care getting medical supplies can be a hassle for caregivers. It requires time, energy, patience and diligence. I remember having to take note of each and every resource to get various supplies, whether it was for dialysis, a wheelchair, or even gauze strips.
According to AARP, nearly 75% of caregivers manage medications and medical tasks. Thomas’ reader Sarah went through a nightmare trying to get the right wheelchair for her husband. “We had to go through so much paperwork and phone calls with the insurance company,” she said.
Shah understands these frustrations. “Partnerships between tech and medical supply companies to streamline this process for caregivers would be super helpful,” he says.
Brown was also a caregiver, and shares her perspective as a provider: “We do our scheduling based on the provider’s schedule, which means working around our own work schedule. We may need to be with our patients when the nurse or home health aide comes. Because of staffing shortages, we often take the schedule that’s given even when the schedule completely derails our day.”
Improving Systems and Patient Satisfaction
Brown says that healthcare professionals can help caregivers and agencies alike by obtaining doctor orders and making effective referrals. “It’s frustrating to have to repeatedly call the doctor’s office to get an order for home health services and durable medical equipment,.” she says.
Source: Printablee
“It’s also important that the healthcare professionals know which providers have staff available. For instance, my dad received home health services with a visiting nurse. When I also asked for a home health aide, the nurse was upfront that there just wasn’t the staff available for home health aide to visit. We could work around that because my sister and I provided my dad’s personal care. Others may not have the luxury, so it’s important to know the reality of what we can expect.
Another thing to consider is the emotional effect on the patient when a provider or aide is no longer available.
For example, there was a week when neither Brown nor her sister would be available on a Friday to care for their dad. “I was waiting to hear if my dad’s home health provider could continue providing services for my dad. I waited to reconfigure my work day on Friday if I needed to provide care. I later heard back from the home health agency that benefits would continue. My dad was worried about benefits ending in part because he had formed a wonderful friendship with his nurse, and he loves her. But the system doesn’t take into account the emotional impact when services end. We miss the care, and we often also miss the care provider.”
Source: EDUCBA
Naama Stauber Breckler, Co-founder of Better Health, is trying to improve accessibility and convenience for people with chronic conditions and dependent on different medical devices and supplies. “Patients need the ability to easily discover and order medical supplies online and get an easy explanation of their insurance benefits, how to maximize them, and how to find the best products,” she says.
Dr. McAllister recommends contacting the insurance company to see what exactly is allowed (HHA, PT, OT, SLP and RN services). “Companies may try to give you less than your family needs, but your insurance company will help you understand what your rights are. Many home health companies are short-staffed, but if you know what you can get for your family member, you will be able to advocate for the best,” she says.
Addressing Caregiver Challenges with Care at Home
Some of the ways to address in-home caregiver challenges include care-at-home and Hospital-at Home programs, using RPM, employer-provided benefits and flexible work arrangements, and better health plan coverage.
The Rise of Hospital-at-Home Programs
Source: Rainbow Health
Care-at-home programs are integrated clinical programs created to deliver healthcare services that have either been traditionally provided within healthcare facilities or represent new care models for chronic disease management.
These programs typically combine remote insight into biometric data or symptoms via connected devices for remote patient monitoring (RPM) and communication with clinicians through telehealth modalities. Many care-at-home programs include in-home services such as durable medical equipment (DME), meal delivery, technical support, and therapeutics.
66% of hospitals and health systems currently offer patients a care-at-home service. Early care-at-home programs were primarily targeted at ad hoc or episodic care, often only relying on a telehealth visit. But the growing maturity of these models and the confidence of the clinical and operational leaders make it increasingly viable to treat chronically and acutely ill patients at home. The differences between these program types include the amount and type of RPM, the in-home services included, and the staffing required to operate the program.
Providing remote care at home can reduce the need for hospital admissions/early discharge, freeing up valuable hospital resources and beds and leaving patients and their families feeling supported in their own homes.
Remote Monitoring for Patients with Chronic Conditions
George’s endocrinologist recommended that he use a Dexcom device to track his blood sugar. This remote monitoring device was great for me because no matter where I was or what time it was, the Dexcom app sent my phone a notification whenever his sugar was too high or too low. It was especially helpful when I attended a conference 6 hours from home, but got his alerts throughout the day and night. His family stayed with him when I was gone, but I got the alerts.
“Remote monitoring technologies have been game-changers for caregivers managing chronic conditions,” Shah says. “… allowing caregivers and clinicians to monitor vital signs and symptoms remotely, providing peace of mind and enabling more proactive care.”
The Current Health platform helps hospitals and clinics provide healthcare services to patients in their homes. Patients can use this platform for various health conditions, including COVID-19, heart problems, pregnancy care, and cancer.
Survey respondents were confident that remote monitoring helps clinicians better understand the patient’s daily health.
Technology is essential to care-at-home programs, but the industry must embrace technology for these programs to be successful. According to another survey by Current Health and Sage Growth Partners, 51% of health system leaders cited patient engagement and adherence as a top challenge, with the most critical support service needs of clinical monitoring (54%), logistics (53%), and technical support (48%). In addition, interoperability between your care-at-home platform and the patient’s employee health record (EHR) is critical for reducing duplicative work for providers and ensuring you have a holistic view of the patient during and after their care-at-home experience.
RPM makes healthcare more accessible, as patients are monitored in their homes. Facing challenges such as high care costs, reduced revenue, and limited capacity, care at home is a cost-effective site of care that can provide better patient outcomes and satisfaction.
Employer Support
Employers can help by providing flexible work arrangements, paid leave, and Employee Assistance Programs (EAPs) that offer counseling, legal help, financial advice, and referrals to eldercare services.
Source: Academy to Innovate HR (AIHR)
In-home caregiving can significantly impact an employee’s ability to manage their work responsibilities. Logan Mallory, VP of Marketing at Motivosity offers flexible work arrangements, like reduced or flexible work hours, to help alleviate the stress of balancing caregiving and work duties. This flexibility allows employees to be present for their loved ones while still fulfilling their work commitments.
Motivosity also offers their employees unlimited paid time off (PTO), health savings accounts (HSAs), and comprehensive health insurance to support our caregiving employees, each of which benefits the employees who are also caregivers in specific ways:
Unlimited PTO ensures that employees can take the necessary time off without worrying about exhausting their leave.
HSAs help cover the costs of medical supplies and services, providing financial relief.
Health insurance plans that cover a wide range of services, including in-home care, which helps employees manage caregiving expenses more effectively. They also provide access to counseling services, stress management resources, mental health apps and gym access.
“While we can only do so much, employers should strive to provide as much support as possible to caregiving employees,” Mallory says. “By offering flexible solutions and understanding their unique challenges, we can help them manage their responsibilities more effectively.”
Health Plan Changes Needed
Insurance Coverage Gaps
Source: Jackson Insurance Brokers
In the U.S., patients and their caregivers could benefit from closing the following health insurance coverage gaps in their health plans:
Long-Term Services and Supports (LTSS): According to theHHS, 70% of people over 65 will require some type of LTSS, which is not covered under Medicare or most private health insurance plans.
Home and Community-Based Services (HCBS): There’s currently limited coverage for services that help with ADLs and care at home.
Caregiver Support Services: Lack of comprehensive coverage for services that directly support family caregivers, such as respite care, training, and counseling in some states.
Non-Expansion States: In states that have not expanded Medicaid, many low-income adults fall into a coverage gap, being ineligible for both Medicaid and Marketplace subsidies (Drake, et al., 2024).
10 Ways Health Plan Changes Can Support Caregivers
Source: Ramsey Solutions
Expand Medicaid Coverage: Adopting Medicaid expansion in all states could provide coverage to approximately 2.9 million uninsured adults, including many caregivers (Drake et al., 2024).
Integrate Caregiver Support: Incorporate caregiver support services into existing health care delivery models and value-based care programs.
Enhance LTSS and HCBS Coverage: Expand coverage for these services under Medicare, Medicaid, and private insurance plans to reduce out-of-pocket costs for families.
Improve Remote Care Options: Expand coverage and availability of remote patient monitoring and telehealth services to support both patients and caregivers. Hospital-at-Home programs should be a mainstay in health plan coverage. These programs are customer-centric, result in lower hospital readmission rates, increase hospital capacity, and reduce issues with resource allocation among clinical staff.
Develop Caregiver-Specific Insurance Products: Create insurance plans or supplemental coverage options designed to meet the unique needs of caregivers.
Enhance Workplace Policies: Encourage employers to offer flexible work arrangements and maintain health insurance coverage for employees who are caregivers (Tingey et al., 2020).
Improve Caregiver Identification and Assessment: Implement systematic processes in healthcare settings to identify, assess, and support caregivers.
9. Include Caregiver Metrics in Quality Measures: Incorporate caregiver experiences and outcomes into healthcare quality measurements to incentivize better support.
Prepare Healthcare Professionals: Enhance training for healthcare providers on person- and family-centered care to better support caregivers. Psychoeducational information (e.g., treatment, lifestyle, etc.) and healthcare (e.g., emotional support, practical services, etc.) were the most common unmet need domains across health conditions (Thomas et al, 2023). Addressing unmet informational or healthcare needs may help optimize outcomes and care for children and families living with common chronic health conditions.
By addressing these gaps and implementing these improvements, the U.S. healthcare system could significantly enhance support for both caregivers and patients by reducing the financial and emotional burden on families while improving overall care outcomes.
Supporting Caregivers and Their Families
Source: Caryfi
As we’ve explored throughout this article, home care programs and RPM offer transformative benefits for both patients and caregivers. These solutions provide enhanced flexibility, improved care coordination, crucial support for managing chronic conditions and reducing caregiver burden. Expanding health plan coverage for these programs is not just beneficial, but necessary.
Hospital-at-Home (HaH) programs, in particular, represent a cost-effective, patient-centered approach that deserves widespread adoption. Every health institution could likely benefit from such a program to increase the capacity of their facility, enhance customer-centricity and patient satisfaction, and promote better patient outcomes. It’s the way of the future, and the way patients want to receive care. So we call on healthcare providers and health plans to prioritize the inclusion of care-at-home programs in their coverage.
By supporting caregivers and improving patient outcomes, we can create a more efficient, compassionate healthcare system. This requires a collaborative effort from healthcare providers, insurers, policymakers, and technology innovators to truly enhance the caregiving experience and, ultimately, the quality of life for both patients and their dedicated caregivers.
References
Carter, K., Blakely, C., Zuk, J., Brittan, M., & Foster,C. Employing Family Caregivers: An Innovative Health Care Model. Pediatrics. 2022; 149(6), 1-4. doi.org/10.1542/peds.2021-054273
“Compensation For Caregiving.” Colorado Respite Coalition, https://coloradorespitecoalition.org/family-caregivers/compensation-for-caregiving.php. Accessed 2 July 2024.
Costa, S., Ferreira, J., Leite, Â., & Pereira, M. G. (2021). Traumatic stress as a mediator of quality of life and burden in informal caregivers of amputees due to diabetic foot: a longitudinal study. Health Psychology Report, 9(4), 339, 345. https://doi.org/10.5114/hpr.2020.101495
Drake, P., Tolbert, J., Rudowitz, R, & Damico, A. “How Many Uninsured Are in the Coverage Gap and How Many Could be Eligible if All States Adopted the Medicaid Expansion?” KFF, 26 Feb. 2024, https://www.kff.org/medicaid/issue-brief/how-many-uninsured-are-in-the-coverage-gap-and-how-many-could-be-eligible-if-all-states-adopted-the-medicaid-expansion. Accessed 2 July 2024.
Fakeye, M.B.K., Samuel, L.J., Drabo, E.F., Bandeen-Roche, K., & Wolff, J.L. Caregiving-Related Work Productivity Loss Among Employed Family and Other Unpaid Caregivers of Older Adults. Value in Health. 2023;26(5):712. https://doi.org/10.1016/j.jval.2022.06.014
Favreault, M., Dey, J., Anderson, L., Lamont, H., & Marton, W. “Future Change in Caregiving Networks: How Family Caregivers and Direct Care Workers Support Older Adults Now and in the Future.” Assistant Secretary for Planning and Evaluation, 2 Aug, 2023, https://aspe.hhs.gov/sites/default/files/documents/a449863a8c93838d37f78ccf29e9231f/future-change-caregiving-networks.pdf. Accessed 2 July 2024.
Fields B., Makaroun L., Rodriguez K.L., Robinson C., Forman J., & Rosland A-M. Caregiver role development in chronic disease: A qualitative study of informal caregiving for veterans with diabetes. Chronic Illness. 2022;18(1):193, 196. doi:10.1177/1742395320949633
“How Caregiving Impacts Families, Communities and Society.” Genworth, 27 Oct. 2021, https://pro.genworth.com/riiproweb/productinfo/pdf/682801BRO.pdf. Accessed 2 July 2024.
Ibrahim N., Chu S., Siau C., Amit N., Ismail R., Halim A., & Gafor, A. The effects of psychosocial and economic factors on the quality of life of patients with end-stage renal disease and their caregivers in Klang Valley, Malaysia: protocol for a mixed-methods study. BMJ Open. 2022;12(6):1-2. doi:10.1136/bmjopen-2021-059305
Katsarou, A., Intas, G., & Pierrakos, G. Investigating the Needs of Caregivers of Patients Suffering from Chronic Diseases: A Mixed-Method Study. Indian Journal of Palliative Care. 2023; 29(3), 285-286. https://doi.org/10.25259/IJPC_179_2022
Khurana, Sanjay. “Caregiver Support | Gaps, Opportunities and Emerging Models in Healthcare.” Linkedin, 19 Oct. 2023, https://www.linkedin.com/pulse/caregiver-support-gaps-opportunities-emerging-models-sanjay-khurana. Accessed 2 July 2024.
Smith, Morgan. “90% of companies say they’ll return to the office by the end of 2024—but the 5-day commute is ‘dead,’ experts say.” CNBC, 11 Sept. 2023, https://www.cnbc.com/2023/09/11/90percent-of-companies-say-theyll-return-to-the-office-by-the-end-of-2024.html. Accessed 26 June 2024.
Thomas S., Ryan N.P., Byrne L.K., Hendrieckx C., White V. Unmet supportive care needs of families of children with chronic illness: A systematic review. Journal of Clinical Nursing. 2023; 32(19-20): 7101. https://doi.org/10.1111/jocn.16806
Tingey, J.L., Lum, J. Morean, W., Franklin, R., & Bentley, J.A. Healthcare Coverage and Utilization Among Caregivers in the United States: Findings From the 2015 Behavioral Risk Factor Surveillance System. Rehabilitation Psychology. 2020; 65(1), 63-71. http://dx.doi.org/10.1037/rep0000307
Umrigar D, Mhaske R. Psychological Health of Wives’ of Patients with Chronic Illnesses. Journal of Psychological Research. 2022;4(1):1-2. doi:10.30564/jpr.v4i1.3879
These platforms are not just fancy apps or websites. From telehealth to AI-powered diagnostics, digital health applications are changing healthcare for the better.
How do these platforms trim the fat from our bloated healthcare system? Let’s explore the ways digital health can make healthcare more affordable for everyone.
Telemedicine brings healthcare right to your home, office, or wherever you are. It’s like having a doctor in your pocket! But how does this convenience translate to cost savings?
Virtual doctor visits reduce travel and waiting room costs
A study published in the Journal of Medical Internet Research found that telehealth visits saved patients an average of 100 minutes of travel time and $50 in travel costs per visit (Snoswell et al., 2020).
Think about the last time you went to the doctor. How much time did you spend traveling and sitting in the waiting room? With telehealth, those time and money costs disappear.
Fewer ER visits
How often have you wondered if that late-night stomach ache was worth a trip to the ER? Telehealth tools like AI chatbots can help you make that decision without leaving home.
Cost savings for both patients and healthcare providers
It’s not just patients who save money. Healthcare providers benefit too. Telehealth services have been found to reduce healthcare costs for providers and patients. Even better, many insurers now have an allowance to cover the cost of certain telehealth visits.
Preventive Care: Stopping Problems Before They Start
Have you ever heard the saying “an ounce of prevention is worth a pound of cure”? Digital health platforms are making this old adage more relevant than ever.
How digital platforms promote healthy habits
From step counters to diet trackers, digital health apps are helping us stay healthier. But do they really make a difference? A study by Ernsting et al. (2017) found that users of health and fitness apps were 34% more likely to meet physical activity guidelines compared to non-users.
Wearable devices and their impact on early detection
Smartwatches surpass the practical use of telling time–they’re becoming powerful health monitors. For example, Apple Watch’s ECG feature can detect atrial fibrillation with 98% accuracy, potentially preventing strokes and saving lives (Perez et al., 2019).
How AI and big data can predict health risks and reduce costs
Big Data Analytics in healthcare uses AI, machine learning and deep learning tools to help doctors find the best treatments for each patient, which can reduce waste. This lets doctors predict health problems and start treatments early, which can save lives. This could change how common certain diseases are and save money on healthcare (Batko & Ślęzak, 2022).
Paperwork is no one’s favorite part of healthcare. Digital platforms are making administrative tasks faster, easier, and more cost-effective.
Automated appointment scheduling and reminders
Have you ever forgotten a doctor’s appointment? Digital reminders can help.
Ulloa-Pérez et al. (2022) found that sending an extra text reminder for high-risk appointments reduced no-shows in primary care and mental health offices, and same-day cancellations in primary care offices.
Targeting reminders using risk prediction models (predictive analytics) can efficiently use healthcare resources, potentially preventing hundreds of missed visits monthly. This approach saves costs compared to messaging all patients, though implementing the risk model has some costs.
Digital health records reduce paperwork and administrative errors
Remember when doctors used to write prescriptions by hand? Digital health records make all kinds of admin work more efficient. A study in the Journal of the American Medical Informatics Association found that electronic health records with AI can reduce medication and billing errors.
Cost savings through improved workflow and resource allocation
Efficient workflows mean better care at lower costs. A study in the Journal of Medical Internet Research found that digital health platforms improved hospital workflow efficiency by 25%, leading to annual cost savings of $1.2 million for a mid-sized hospital (Luo et al., 2019).
Data-Driven Insights for Better Decision Making
In the age of big data, information is power. Healthcare is no exception. With all this digital information, doctors can make smarter choices about your health.
How big data analytics improve treatment plans
A study in the Journal of Big Data found that big data analytics improved treatment efficacy by 30% and reduced treatment costs by 20% (Dash et al., 2019).
Cost savings from shorter and fewer hospital stays
Have you ever wondered how hospitals decide how many beds they need? Predictive analytics is the answer. It can reduce hospital bed shortages and decrease operational costs.
Hospital stays are expensive, but RPM can help shorten them. RPM allows patients to be discharged an average of 2 days earlier, resulting in cost savings of $7,000 per patient.
Personalized medicine and its impact on cost reduction
One size doesn’t fit all in healthcare. Targeted treatments are more effective and cost-effective.
Personalized treatment plans based on genetic data improve treatment efficacy and reduce adverse drug reactions (ADRs).
Nobody likes going back to the hospital. Remote monitoring can help prevent that. A study in the New England Journal of Medicine found that remote monitoring reduced hospital readmissions for heart failure patients by 50% (Perez et al., 2019).
Management of chronic conditions from home
Chronic conditions are a major driver of healthcare costs. Remote monitoring can help manage these conditions more effectively.
Specialized care can be hard to access, especially in rural areas. Digital health isn’t just about general care – it’s also bringing expert help to more people.
Telehealth solutions for rural and underserved areas
Rural healthcare access is a major challenge. Telehealth can help bridge that gap. A study in Health Affairs found that telehealth increased access to specialty care in rural areas by 54%.
Telehealth also faces challenges like high setup costs and outdated payment models, especially in rural areas. Its success depends on cost distribution, clinical outcomes, and indirect savings. Hospitals need funding and strategies to reach underserved groups and ensure fair access to telehealth (Anawade et al., 2024).
Virtual second opinions and their impact on treatment decisions
Getting a second opinion can be life-changing. Virtual platforms make it easier than ever. Virtual second opinions can change the diagnosis or treatment plan in over one-third of cases, potentially avoiding unnecessary procedures and costs.
Conclusion
Digital health platforms are powerful allies to counteract rising healthcare costs. By leveraging technology for prevention, efficiency, and data-driven insights, these platforms are making healthcare more accessible and affordable. From applications like telehealth reducing unnecessary ER visits to catching illnesses early with AI-powered diagnostics, the potential for cost savings is huge.
As patients, we can embrace these digital tools to take control of our health and potentially lower our healthcare expenses. For healthcare providers, adopting these platforms could lead to more efficient operations and better patient outcomes.
What do you think about these digital health innovations? Have you used any of these technologies in your own healthcare journey?
References
Anawade, P. A., Sharma, D., & Gahane, S. (2024). A Comprehensive Review on Exploring the Impact of Telemedicine on Healthcare Accessibility. Cureus, 16(3). doi.org/10.7759/cureus.55996
Batko, K., & Ślęzak, A. (2022). The use of Big Data Analytics in healthcare. Journal of Big Data, 9(1). doi.org/10.1186/s40537-021-00553-4
Dash, S., Shakyawar, S. K., Sharma, M., & Kaushik, S. (2019). Big data in healthcare: Management, analysis and future prospects. Journal of Big Data, 6(1), 1-25. doi.org/10.1186/s40537-019-0217-0
Ernsting, C., Dombrowski, S. U., Oedekoven, M., & Kanzler, M. (2017). Using smartphones and health apps to change and manage health behaviors: A population-based survey. Journal of Medical Internet Research, 19(4), e101.
Grand View Research. (2024). Digital Health Market Size, Share & Trends Analysis Report By Technology (Healthcare Analytics, mHealth), By Component (Hardware, Software, Services), By Application, By End-use, By Region, And Segment Forecasts, 2024 – 2030. Retrieved from https://www.grandviewresearch.com/industry-analysis/digital-health-market
Luo, L., Li, J., Liang, X., Zhang, J., & Guo, Y. (2019). A cost-effectiveness analysis of a mobile-based care model for community-dwelling elderly individuals. Journal of Medical Internet Research, 21(5), e13563.
Perez, M. V., Mahaffey, K. W., Hedlin, H., Rumsfeld, J. S., Garcia, A., Ferris, T., Balasubramanian, V., Russo, A. M., Rajmane, A., Cheung, L., Hung, G., Lee, J., Kowey, P., Talati, N., Nag, D., Gummidipundi, S. E., Beatty, A., Hills, M. T., Desai, S., … Turakhia, M. P. (2019). Large-scale assessment of a smartwatch to identify atrial fibrillation. New England Journal of Medicine, 381(20), 1909-1917.
Prasad Vudathaneni, V. K., Lanke, R. B., Mudaliyar, M. C., Movva, K. V., Kalluri, L. M., & Boyapati, R. (2024). The Impact of Telemedicine and Remote Patient Monitoring on Healthcare Delivery: A Comprehensive Evaluation. Cureus, 16(3). doi.org/10.7759/cureus.55534
Snoswell, C. L., Taylor, M. L., Comans, T. A., Smith, A. C., Gray, L. C., & Caffery, L. J. (2020). Determining if telehealth can reduce health system costs: Scoping review. Journal of Medical Internet Research, 22(10), e17298.
Ulloa-Pérez, E., Blasi, P. R., Westbrook, E. O., Lozano, P. , Coleman, K. F., & Coley, R. Y. (2022). Pragmatic Randomized Study of Targeted Text Message reminders to Reduce Missed Clinic Visits. The Permanente Journal, 26(1), doi/10.7812/TPP/21.078
In today’s fast-paced world, staying on top of your health can be a challenge. Why not use your smartphone as your personal health assistant? Whether you’re looking to manage a chronic disease or simply keep track of your fitness goals, there’s an artificial intelligence (AI) health app for that.
44% of smartphone users have at least one health app installed (Beckham, 2024) and use it to track and analyze their well-being. Let’s explore the top 10 best AI health apps changing the game in personal wellness management, and how to decide which one’s best for you.
AI health apps are more than just fancy gadgets. They leverage machine learning (ML) algorithms to analyze data from various sources, such as wearable devices, medical history, and biometric data.
Benefits of Using AI for Health-Tracking
Why should you consider using an AI health app? Smartphones and smartwatches can keep track of your health using AI to analyze your health data and monitor everything from your heart rate to your sleep patterns, helping you stay on top of your health. A few more compelling reasons include access to:
Remote Patient Monitoring (RPM): These apps allow healthcare providers to track their patients health offsite, making healthcare more accessible.
Convenience: With everything in one app, you can easily track your health metrics, set wellness goals, and receive medication reminders.
An AI health app can track your physical activity, monitor your heart rate, and even analyze your sleep patterns. This info can help you understand your overall health better and make informed decisions.
With so many options available, it’s important to know what features make a great AI health app.
What to Look for in Health Apps
When choosing an AI health app, it’s essential to know what features to look for. Here are some must-have features:
Activity Tracking: Monitor your daily physical activity, including steps taken, calories burned, and workout intensity.
Heart Rate Monitoring: Keep track of your heart rate during different activities and rest periods.
Sleep Tracking: Analyze your sleep patterns to improve your sleep quality.
Nutrition Tracking: Log your meals and monitor your calorie intake.
Symptom Checker: Identify potential health issues based on your symptoms.
Medication Reminders: Get reminders to take your medications on time.
User-Friendly Interface: Easy to navigate and use, even for non-tech-savvy users.
These features can help you manage your health more effectively and make the app a valuable tool in your daily life.
Now that we know what to look for, let’s explore some of the top AI health apps on the market.
Our Picks: The 10 Best AI Health Apps
1. MyFitnessPal
MyFitnessPal, developed by Under Armour, is a health app that focuses on nutrition and fitness tracking. It helps users log their meals, track their calorie intake, and monitor their physical activity.
Key Features:
Calorie counter
Nutrition tracking
Exercise tracking
Integration with other fitness apps and devices
Pros
Cons
Extensive food database
Ads in the free version
User-friendly interface
Some features require a premium subscription
Use Case
Ideal for individuals looking to manage their diet and fitness goals.
Fitbit, now owned by Google, is a well-known name in the fitness tracking industry. The app works with Fitbit wearable devices to monitor various health metrics.
Key Features:
Activity tracking
Heart rate monitoring
Sleep analysis
Personalized health insights
Pros
Cons
Comprehensive health-tracking
Requires a Fitbit device
User-friendly interface
Some features require a premium subscription
Use Case
Suitable for fitness enthusiasts who want a detailed analysis of their health metrics.
Headspace is a mental health app that focuses on meditation and mindfulness. It helps users manage stress, improve sleep, and enhance overall well-being.
Key Features:
Guided meditation sessions
Sleep sounds and bedtime stories
Stress management tools
Personalized recommendations
Pros
Cons
High-quality content
Subscription required for full access
User-friendly interface
Limited free content
Use Case
Great for individuals looking to improve their mental health and reduce stress.
Samsung Health is a versatile health app available for Android and iOS devices. It tracks various health metrics and offers personalized health insights.
Key Features:
Activity tracking
Heart rate monitoring
Sleep analysis
Stress management tools
Pros
Cons
Wide range of features
Some features require Samsung devices
User-friendly interface
Ads in the free version
Use Case
Ideal for Samsung device users looking for a detailed health-tracking app.
Garmin Connect works with Garmin wearable devices to provide detailed health and fitness tracking. It shows data about your physical activity, sleep, and more.
Key Features:
Activity tracking
Heart rate monitoring
Sleep analysis
Workout planner
Pros
Cons
Detailed health insights
Requires a Garmin device
Customizable
Some features are complex
Use Case
Best for athletes and fitness enthusiasts using Garmin devices.
Try Free Versions: Many apps offer free versions or trials. Test them out before committing to a subscription.
By considering these factors, you can find an app that meets your health-tracking needs and fits seamlessly into your lifestyle.
While these apps can be incredibly helpful, it’s crucial to consider how they handle your personal information.
Privacy and Security Considerations
When it comes to health apps, privacy and security are paramount. Here are some key considerations (ERTech, 2023):
Data Encryption: Ensure the app uses encryption to protect your data during transmission and storage.
Secure Authentication: Look for apps that offer multi-factor authentication to verify your identity.
Clear Privacy Policies: The app should have a transparent privacy policy that is easy to understand.
Data Sharing: Be cautious of apps that share your data with third parties, especially for advertising purposes.
A study in the British Medical Journal found that many health apps have serious privacy issues, including a lack of transparency in their privacy policies (Grundy et al., 2019). It’s crucial to choose apps that prioritize your data privacy and security.
As exciting as current AI health apps are, the future holds even more promise. Let’s take a look at what’s coming.
The Future of AI in Health Monitoring
The future of AI in health monitoring looks promising. Here are some trends to watch:
Advanced Predictive Analysis: AI will become better at predicting health issues before they occur, leading to more proactive healthcare.
Integration with Telemedicine: AI health apps will work more seamlessly with telemedicine services, providing a well-rounded healthcare solution.
Personalized Healthcare: AI will continue to offer more personal tips tailored to individual needs and preferences.
Improved Data Privacy: As privacy concerns grow, AI health apps will adopt more advanced privacy-preserving techniques, such as federated learning and differential privacy (Yadav et al., 2023).
AI health monitoring apps are powerful tools that put wellness management at your fingertips. From tracking your sleep patterns to monitoring your heart rate, these smart applications offer personalized insights to help you make informed decisions about your health.
Remember, while these apps are incredibly useful, they’re not a replacement for professional medical advice. Use them as a complement to regular check-ups and always consult with your healthcare provider for serious concerns. By choosing the right app and prioritizing privacy and security, you can take control of your health and well-being.
Grundy, Q., Chiu, K., Held, F., Continella, A., Bero, L., & Holz, R. (2019). Data sharing practices of medicines related apps and the mobile ecosystem: Traffic, content, and network analysis. BMJ, 364, l920. doi.org/10.1136/bmj.l920
Yadav, N., Pandey, S., Gupta, A., Dudani, P., Gupta, S., & Rangarajan, K. Data Privacy in Healthcare: In the Era of Artificial Intelligence. Indian Dermatology Online Journal, 14(6), 788-792. doi.org/10.4103/idoj.idoj_543_23