
Your patients don’t stop using your product because it’s bad. They disengage because no one taught them how to use it, nor explain why they should.
I didn’t come to patient education content through a certification program or a content strategy course. I came to it through a stack of medical devices on my nightstand, a peritoneal dialysis machine running in my living room every night, and the slow realization that every piece of content we received about managing George’s conditions had been written for someone who wasn’t us.
Not because we weren’t capable. Because we were overwhelmed — and nobody who wrote that content had accounted for the difference.
I’ve thought about that a lot since I started writing onboarding and education content for healthtech companies. The information existed. The problem was never the information. Someone just packaged it for a patient who doesn’t survive a serious diagnosis intact.
Contents
The issue with a drip sequence
Most healthtech SaaS companies solve the post-signup silence with a drip sequence where:
- A welcome email goes out on Day 0.
- Something like “here’s what you can do with the platform” follows on Day 3.
- A check-in on Day 7.
The sequence runs automatically, open rates look fine, and then the team moves on to the next.
Drip sequences were built for marketing to move a prospect through a funnel, warm them up before a sales conversation, and keep a brand top of mind.
They’re timed and trigger-based. They’re also written for someone who has attention to spare. Not a patient living with 3 chronic conditions, and trying to figure out why their reading looks wrong.
The assumptions inside a standard drip sequence don’t hold up in a patient onboarding context. The assumption that information delivered on a schedule gets absorbed on that same schedule. The assumption that a “next steps” email sent on Day 7 will be acted on by Day 8. The assumption that if you include the information, people will find it.
None of that is how it works when someone is exhausted, managing competing health priorities, and staring at a device they don’t fully understand yet.
What an educational email course does differently

Here’s the difference:
- A drip sequence asks: when should we contact this user?
- An educational email course asks: what does this person need to understand to succeed, and in what order?
That difference changes the structure, the language, the pacing, and honestly, the results.
Each email has one job—one specific action the patient can complete within 5 minutes. The sequence is built so that Day 1 makes Day 2 easier, and Day 2 makes Day 3 make sense.
The patient is being walked through a process, not nudged along a timeline.
The language is written for a real person managing a real condition, not an ideal user who has time, focus, and a high health literacy. But in the US, 9 out of every 10 adults struggle to understand healthcare and the resources available to them.
That’s almost everyone who uses your product. If your onboarding assumes otherwise, you’re starting with a comprehension gap you’ll never close.
The communication problem runs deeper than literacy alone. According to the 2026 State of Patient Communications Report, 87% of providers rate their patient-facing technology as up to date. But only 25% of patients report receiving multiple proactive outreach attempts from their provider in the past year.
Providers believe they’re communicating. Patients aren’t experiencing it that way. That’s not a technology failure. That’s a content and sequencing failure, and it shows up in the same activation data you’re already tracking.
Critically, each email explains why patients should do what they’re being asked to do. Instead of just saying “take your blood pressure twice daily,” explain that twice-daily readings produce the pattern data your care team needs to catch a problem before it becomes an emergency.
Patients who understand the reason behind an action are significantly more likely to do it consistently.
Medication adherence research has documented this for decades. The same principle applies to every health behavior your product depends on.
Which version works better?

Here’s an example with 2 versions of the same onboarding instruction for an RPM blood pressure monitor:
- Version A: “Ensure proper cuff placement at heart level for accurate systolic and diastolic readings.”
- Version B: “Wrap the cuff around your upper arm so the bottom edge sits about an inch above your elbow. The tube should line up with the inside of your arm. Sit quietly for 5 minutes. Even a short walk can affect your reading.”
It’s the same information. Version A passes regulatory review, but Version B is the one people can actually follow.
The patient who reads Version A and gets a confusing number will assume they did something wrong, feel embarrassed about it, and probably not try again. The patient who reads Version B has enough context to troubleshoot on their own.
That’s the difference between content written for compliance and content written for comprehension. (You can be both, by the way. It just takes more effort.)
How PX problems affect your business
Patient engagement isn’t abstract for a Series A or B healthtech company. The patient experience (PX) shows up in:
- Contract renewal discussions
- The number of re-onboarding calls your customer success team has to field
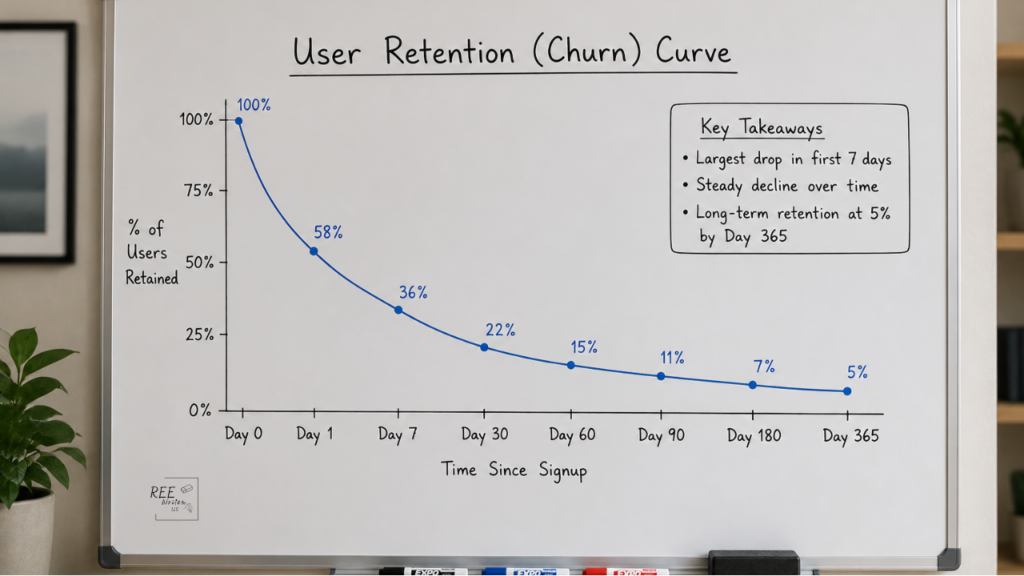
- Churn
When patients don’t activate your device, or when they half-set-up the device and drift away, the cost lands somewhere—on your CS team, your NPS score, and eventually your retention numbers.
A well-built educational email course is cheaper than all of that. It also isn’t a knowledge base article, an in-app tooltip, or a PDF in the resource center that nobody opens. It’s a structured sequence that meets patients where they already are — in their inbox in plain language, in the right order, at the right moment.
Most healthtech companies haven’t built one. That gap is not small.
The companies that avoid these issues asked a different question: “Did anyone understand our email well enough to act?”
That question changes everything downstream: the structure, the language, the sequence, and ultimately whether the patient who needed the product most ever got anything out of it.